
Rewiring Neurogenic Dysphagia:
Finding Hope in the Brain-Swallow Connection
Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction
This June, for Dysphagia Awareness Month we are embarking on a four-week journey to discover the complexities of swallowing. To start, we aren’t looking at just the mouth, throat or esophagus; we are looking at the Controller ~ the brain and nervous system. When this system is out of control, it can cause neurogenic dysphagia.
When we think of swallowing, we often think of the physical act of chewing or chugging water. However, for those living with neurogenic dysphagia, the struggle doesn’t start in the muscles — it starts in the neural pathways. This can cause difficulty swallowing in the oral, pharyngeal, and esophageal dysphagia phases (aka, oropharyngeal dysphagia and pharyngoesophageal dysphagia). Please see my blog from last week, introducing Dysphagia Awareness Month with its review of these phases of the swallow.
Whether it is a sudden “software crash” like a stroke or a “system slow-down” like Parkinson’s Disease, the neurological side of swallowing involves complexities that would fill many programming manuals. Allow me to give you a quick reference guide here.
What is Neurogenic Dysphagia?
Simply put, neurogenic dysphagia is a swallowing impairment caused by damage to the central nervous system (the brain and spinal cord) or the peripheral nervous system (the nerves that carry signals to the muscles).
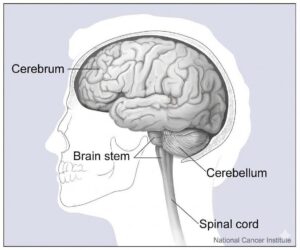
Swallowing is one of the most complex tasks the human body performs. It requires the precise timing and coordination controlled by the cortex, the subcortex, cerebellum, and brainstem, sending out messages to over 5 different cranial nerves involved with swallowing and over 50 pairs of muscles. It is a perfectly coordinated sequence that lasts less than two seconds. When the neurological “wiring” is damaged, our body’s sensory inputs and motor outputs can be affected. Brain damage has the potential to disrupt the swallow’s timing, coordination, and strength.
The Anatomy of a Masterpiece: How the Brain Controls the Swallow
To understand why neurogenic dysphagia occurs, let’s simplify the process into three of the main “stations” of the swallowing circuit: the cortex or cerebrum, the brainstem, and the cranial nerves/peripheral nerves. The cerebellum and spinal cord are certainly involved too, but this is a simplification.
1. The Cortex: The Decision Maker
The “voluntary” part of your swallow starts in the cerebral cortex (cerebrum). The cortex gives you control.
The cortex helps you recognize that it is food in your mouth and not a pill or another object. Damage here may look like a person spitting out a pill or starting to chew it, as they don’t recognize that it is something to swallow whole.
The cortex helps you plan and problem solve. You decide how big of a bite to take, how fast to go, and how much chewing is needed. You break down the food into a manageable ball (bolus) and push the bolus to the back of the mouth when it is swallow ready. That takes a lot of processing, attention, and planning ~ that is the brain thinking!
However, we take that process for granted – as the part of the swallow that is under our control (by the cortex) seems so automatic – until something goes wrong.
Damage up in the cortex — from a stroke, Traumatic Brain Injury (TBI), or Dementia — can lead to all sorts of problems, from food falling out of the mouth to forgetting how to start the swallow. This is known as swallow apraxia or the inability to plan and start a skilled movement, which can happen from a stroke or dementia (see sections below). Imagine, forgetting how to complete a task that has seemed so automatic all our life! We usually don’t think about all the incoming sensory input that starts the good motor output of our swallow.
2. The Brainstem: The Engine Room
Speaking of the most basic sensory input to motor output loops, we must think about the brainstem. Specifically, it is the medulla that houses the Central Processing Generator (CPG). The CPG includes the interconnected network: nucleus solitarius, reticular formation, the nucleus of the crucial cranial nerve X (ten), and nucleus ambiguus. We can think of this as the medullary swallowing center. This is the autopilot of the swallow. Once you send the bolus over the back of the tongue into the throat, the brainstem takes over, triggering the pharyngeal swallow response and the pharyngeal phase of the swallow. Again, see my prior blog on the phases of the swallow here.
Special Section on Wallenberg Syndrome:
For a deeper dive into the impacts of a brainstem stroke at the level of the swallow center, please see my 2014 article on Wallenberg Syndrome (aka, Lateral Medullary Syndrome or Lateral Medullary Infarct) in SwallowStudy.com resources. Please also see the 2019 research from Dr. Mari Nakao and colleagues on the disruptions that occur in the swallowing sequence.
A Lateral Medullary Infarct (aka, Wallenberg Syndrome) is a stroke that is often misdiagnosed or missed all together. It may start with dizziness, nausea and vomiting, as well as an unsteady gait/walking, drooping in one eye, hoarseness, and difficulty swallowing. These signs of Wallenberg Syndrome (see chart below) are not like typical strokes in which the public recognizes the acronym of FAST, which stands for: Face drooping, Arm weakness, Speech/Swallow Difficulty, and Time to call 911. (See my prior article on post-stroke dysphagia and importance of acting quickly)
Wallenberg Syndrome comes with a cluster of symptoms, and this is why this type of stroke is called a syndrome. Please see Table 1 from my 2014 article:
| Signs | Structures affected |
|---|---|
| Ipsilateral loss of pain and thermal sense over half of face | Spinothalamic tract and descending nucleus and tract of cranial nerve V |
| Ataxia, falling to side of lesion | Inferior cerebellar peduncle, spinocerebellar tract |
| Ipsilateral Horner’s syndrome (constricted pupil, ptosis, decreased sweating) | Descending sympathetic tract |
| Dysphagia, dysarthria, ipsilateral paralysis of palate and vocal cord, diminished ipsilateral gag reflex | Efferent fibers of cranial nerves IX and X, and nucleus ambiguus (NA) |
| Contralateral impaired pain and thermal sense below the neck (UE and LE) | Spinothalamic tract and nucleus of cranial nerve V carrying pain and temperature sense to the opposite side of the body |
| Vertigo/dizziness | Vestibular nuclei and vestibulocerebellar pathway in the inferior cerebellar peduncle (J.S. Kim, 2000) |
| Nausea/vomiting, nystagmus, diplopia | Vestibular nuclei (J.S. Kim, 2000) |
If you know anyone who has had a lateral medullary stroke (Wallenberg Syndrome), you know how devastating damage to the lateral medulla can be. It can completely disrupt the pharyngeal swallow sequence, and Dr. Huckabee (2014) and Dr. Nakao’s (2019) research has discussed this “pharyngeal mis-sequencing.” This leaves the airway wide open and unprotected, while the upper esophageal sphincter does not relax and open to allow the bolus to pass into the esophagus. Due to major safety and efficiency problems, the person often does not have a functional swallow for food, liquid, pills, or even saliva. Their voice may sound wet-gurgly. They may constantly need to spit out their saliva or require an oral suction to help clear it. However, as I noted in my article on SwallowStudy.com from 2014, recovery tends to be good within the first 3 months post-stroke with comprehensive neurogenic dysphagia evaluation and management!
Again, it is essential to act FAST for any type of sudden difficulty in your voice, speech, and/or swallowing, as the faster you receive advanced care at a hospital, the better!
3. The Cranial Nerves: The Messengers
The “Big Five” cranial nerves (Trigeminal, Facial, Glossopharyngeal, Vagus, and Hypoglossal) act as the delivery drivers for:
- Bringing in sensory information (e.g., taste, size, temperature, allowing your cortex to decide: “this bite is too big” or “this soup is too hot”); and
- Sending out motor commands to the muscles (e.g., a patterned sequence that can even adjust based on the size of the food: “swallow with a little more force on that big bite of steak”).
Please see my article and chart for these crazy cranial nerves – especially for clinicians who need to nerd out for that board certification exam! For example, make sure you know that the nerve nucleus of the Facial Nerve, CN VII comes out of the pons. Therefore, a pontine stroke can cause facial paralysis. Did you know that a person who lacks the sense of pain and temperature (test with those ice cubes from the hospital floor’s nourishment kitchen) may have an issue in the upper medulla at the level of a sensory branch of the Trigeminal Nerve, CN V? The speech pathologist’s thorough oral sensory-motor exam at the bedside covers all these cranial nerves and can provide crucial neurological information for the neurologist’s differential diagnostic process!
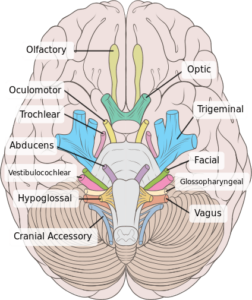
See the cranial nerves potentially involved in neurogenic dysphagia, such as the Trigeminal, Facial, Glossopharyngeal, Vagus, and Hypoglossal. These come out of the pons and medulla, which you see here looking at the undersurface of the brain.
5 Common Culprits: Who is Affected by Neurogenic Dysphagia?
Because so much of the brain is involved in swallowing, many different neurological conditions and diseases can lead to neurogenic dysphagia (in oropharyngeal and pharyngoesophageal phases). This is a very simplified introduction to 5 common areas representing the underlying causes of neurogenic dysphagia.
1. The Sudden Impact: Stroke and Traumatic Brain Injury
Stroke is perhaps the most common cause of neurogenic dysphagia. When reviewing the literature, one can find any percentage of prevalence of dysphagia in stroke from 37% to 80%. So, how much of a concern is post-stroke dysphagia?
As noted by Dr. Martino and colleagues (2005), it depends on if the person has a comprehensive dysphagia evaluation or not! She noted:
“The reported incidence of post-stroke dysphagia was lowest using cursory screening techniques (37% to 45%), higher using clinical testing (bedside swallow by SLP) (51% to 55%), and highest using instrumental testing (64% to 78%).
Depending on the location of the stroke, a patient might experience different symptoms, but one common issue is a delayed swallow trigger or initiation. It is important to identify dysphagia risk quickly in post-stroke care at the hospital. We have long known that symptoms such as hoarseness (dysphonia), slurred speech (dysarthria) correlate strongly with risks for dysphagia (Daniels et al., 1997).
Early nursing swallow screening is essential prior to giving anything by mouth (i.e., even medications with sips of water could be risky). Please see this blog reviewing Dr. Steven Leder’s work with colleagues to develop nursing swallow screening protocols (Yale Swallow Protocol). Screening is the first step, but the reason for the screen is to quickly trigger a referral to the speech-language pathologist (SLP) for a comprehensive dysphagia evaluation and intensive dysphagia management. Medical SLPs help people regain function and quality of life.
As I noted in my blog about stroke and dysphagia risk management from 2017, the medical team needs to consider the lesion location and type as risk factors prior to ordering any food, liquid or medications by mouth. The following lesion sites and types of strokes can be predictive of dysphagia:
- Supratentorial strokes (top half of the brain, including the cortex and subcortex): specifically in the insula, primary somatosensory, primary motor, and motor supplementary areas, orbitofrontal cortex, internal capsule, putamen, caudate nucleus, basal ganglia (Gonzalez-Fernandez et al., 2008; Saito et al., 2016; Im et al., 2018)
- Infratentorial strokes (lower half of the brain of the cerebellum and brainstem structures): pontine, medial medullary, lateral medullary (Flowers et al., 2011 & 2017). Again, see my post and paper on Lateral Medullary Syndrome.
- Hemorrhagic strokes
- Large and Multiple lesions, especially when in both hemispheres (i.e., bilateral strokes).
People with cortical strokes in the right hemisphere (in right-handed people) may have additional issues that reduce the person’s safety while eating and drinking. They may have neglect (not attending to) the entire left side of their body, the room, or even the tray of food in front of them. They may not believe that they have any deficits and want to walk out of the hospital. We may also see these types of poor self-awareness issues in the people with traumatic brain injury (TBI).
The sudden impact of a traumatic brain injury and other types of brain injury can disrupt many levels of the brain and spinal cord, severely disrupting the swallow at any stage. The person may have required prolonged intubations and an extended time of being fed by a feeding tube — further impacting their sensation, muscles, timing, and coordination of the swallow. Additionally, attention, cognitive, executive function (i.e., ability to plan, multitask, organize, and focus attention to complete tasks) difficulties are common. These reduce the person’s self-awareness of their difficulties, ability to predict risks, and skill in solving problems. Often the person is agitated and impulsive, which may cause eating too fast and taking too large of bites. Behavioral issues from certain types of strokes and TBI can increase choking/airway obstruction risks.
2. The Movement Disorders: Too Little or Too Much Movement?
Movement Disorders may cause reduced movement (hypokinetic) or a slowness of movement (bradykinetic). Other disorders, not addressed here, cause the opposite of too much movement (hyperkinetic).
Parkinson’s Disease is the most common movement disorder, but sometimes people only have features of this disease, called Parkinsonism (see this blog about the extrapyramidal side-effects that can occur with many antipsychotic medications as an example of Parkinsonism). Also not addressed in this blog are the numerous Parkinson’s Plus Syndromes. These are diseases, such as progressive supranuclear palsy (PSP), that are often identified after a person does not respond to typical Parkinson’s medications.
Parkinson’s Disease (PD): Specific issues with swallowing in Parkinson’s may be related to rigidity and bradykinesia (slowness of movement). Tremors may make feeding oneself challenging. Additionally, difficulty with divided attention (when faced with multi-tasking or distractions) may cause reduced attention of the need to swallow saliva, resulting in pooling of saliva in the mouth and drooling (Reynolds, Miller & Walker, 2018). The oral phase may show the tongue “rocking” the food back and forth (repetitive lingual pumping) prior to propelling the food backward. This is similar to the rocking a person may do to initiate standing up from a chair. The tongue’s propulsion and the throat’s squeezing action may be weak, leaving food, liquid, or pills stuck in the throat. The overall speed and strength of airway closure may also be impaired, causing liquid to go down the wrong way. Furthermore, people with Parkinson’s often have reduced sensation, meaning they may not even feel food sitting in their throat, realize they are aspirating, or have an urge to cough.
Dr. Christina Pflug’s 2018 research in Parkinson’s Disease indicates that 95% of People with PD exhibit some objective swallowing difficulty when tested with instrumental swallowing studies (MBSS/VFSS or FEES). Past research on prevalence typically used only questionnaires or scales to ask the person if they feel a swallowing problem, but PD affects the sensation and awareness of dysphagia. In those with difficulty clearing solid foods, bread posed the highest risk for dangerous residue in the throat. Pflug’s research showed that only 5% of individuals with PD had normal function. The study also found that 16% of patients with no reports of difficulty swallowing were actually having silent aspiration (i.e., liquids getting down the wrong way and not feeling it at all or not having an urge to cough).
Much research has been conducted on the “blunted urge to cough” found in people with Parkinson’s (i.e., please search for work by Drs. M. Troche, A. Brandimore, K. Hegland, and many more. See Dr. Troche’s Laboratory for the Study of Upper Airway Dysfunction for one resource).
3. The Nerve – Muscle Disconnect: Neuromuscular Disorders & Diseases
This is a very large group, which has multiple subcategories. Please see a course on the American Board of Swallowing and Swallowing Disorders (AB-SSD) website within their 2025 Summer Series, titled: “Dysphagia in Neuromuscular Disease: Unique Considerations for Patient-Centered Care.” The speaker, Sarah Stranberg, MA, CCC-SLP, offered these main subcategories (not a complete list):
- Muscular Dystrophies (e.g., Duchenne muscular dystrophy, oculopharyngeal muscular dystrophy): weakness in the skeletal/striated muscles themselves.
- Motor Neuron Disease (e.g., Amyotrophic Lateral Sclerosis/ALS and Spinal Muscular Atrophy/SMA): can affect upper and lower motor neurons resulting in weakness of muscles. I like how AI described this: “the main circuit breakers are burning out.”
- Neuromuscular Junction Diseases (e.g., Myasthenia Gravis): problem in the “protein transmission of signals,” per Stranberg, to the muscles themselves. Remember those acetylcholine receptors from biology class? AI described: “the wall outlets are broken.”
- Myopathies (e.g., Inclusion Body Myositis/IBM, Dermatomyositis): muscle fibers are not functioning.
- Mitochondrial Diseases (e.g., Friedreich’s Ataxia): mutations inside the mitochondria impairing cellular energy production (ATP).
- Peripheral Nerve Diseases (e.g., Charcot-Marie-Tooth disease): problem outside the central nervous system in the peripheral nerves.
One example of a neuromuscular disease that causes significant neurogenic dysphagia is:
Amyotrophic Lateral Sclerosis (ALS or “Lou Gehrig’s Disease”) attacks the motor neurons themselves. In bulbar-onset ALS, the muscles of the mouth and throat are affected early, making speech, swallowing, and airway protection primary concerns. The management of saliva and the safe and efficient intake of foods, liquids, and pills may become a significant struggle. At least 85% of people with ALS (also known as PALS) will experience dysphagia in the course of the disease (Plowman, 2015). Only a small percentage of people researched will maintain both a safe and efficient swallow (Robinson et al., 2022). Please recall the descriptions of safety (no aspiration) and efficiency (no residue buildup after the swallow) in my prior blog. Please see these important resources for people with ALS (PALS):
4. The Master Control Disconnect: Multiple Sclerosis (MS)
This is different from the neuromuscular disorders/diseases above, as it affects the central nervous system and is an autoimmune attack on the central nervous system’s myelin sheath (insulation around the nerve lines and tracks). (Note: MS is different from the autoimmune issues in Myasthenia Gravis above).
This is an inflammatory disease process blocking the path/route of signals through the brain and spinal cord, and not a primary attack on the actual nerve cells or the junctions of nerve and muscle (like in neuromuscular junction disease of Myasthenia Gravis). Again, an AI analogy to the rescue: MS is like having “the rubber insulation stripped away on the high-voltage transmission lines that leave the master control facility, causing short circuits before the signal leaves the building to the home.”
Neurogenic Dysphagia in people with MS is one of the most common issues that affect quality of life and mortality in the later stages (Aghaz et al, 2018). Because we cannot provide enough details here on this chronic neurological and autoimmune disorder and all its types, please see other resources:
- National Multiple Sclerosis Society
- NIH Health Information on Multiple Sclerosis (MS)
- Mayo Clinic Multiple Sclerosis
5. The Slow Decline: Alzheimer’s Disease & Related Dementias
For a person in the advancing stages of Alzheimer’s Disease or other Related Dementias (ADRD), there is damage to areas of the cortex and limbic system causing losses in:
- memory (immediate recall, working memory, procedural memory in how to complete common activities of daily living/ADLs, and eventually long-term memory),
- cognitive functions (orientation – such as knowing your location, reasoning, sustained attention, speech-language skills, executive function, etc.), and
- regulation of emotion and personality.
Swallowing may be the last activity of daily living to decline in the end of these terminal diseases. The person may no longer be able to feed themselves, but they are still swallowing. They may not recognize how to use a spoon, but with feeding assistance, the automatic nature of the swallow may still allow them to continue to eat familiar soft foods and favorite drinks until the more severe to profound stages.
A caregiver can maximize this automatic nature of the swallow by trying hand-over-hand assistance to help the person hold their own cup. The act of the person bringing their cup up to their mouth uses the more automatic sensory to motor loop to overcome that swallow apraxia discussed above. That may encourage a more normalized sip-swallow (suck-swallow) pattern that the body has done since birth. The more someone becomes dependent on others for feeding and cleaning their mouth, the higher the likelihood is of developing aspiration pneumonia (per predictors from landmark research by Langmore et al., 1998 & 2002).
See another blog here about caregiver burden and resources when caring for a person with dementia.
Dysphagia is very common in people with Alzheimer’s Disease and related dementias, but the statistics may be highly variable depending on when in the disease process a person was tested and how they were tested. The prevalence may be as high as 84-93% in those in the moderate to severe stages (Mira et al., 2022), whereas, it may affect 100% of those with very advanced/end-stage disease. Afterall, unfortunately, these Dementias are terminal illnesses and often ends with the inability to swallow and/or recurrent aspiration pneumonias. Placing a feeding tube in a person at that end-stage is not appropriate and may lead more quickly to aspiration pneumonia, rather than trying to prevent it. Overall, tube feeding is contraindicated (not advisable), but that full discussion is not the focus of this article. Please see this article about important conversations to have regarding a person’s goals of care and palliative care.
For speech pathologists who support people with dementia, please see this course by Dr. Nicole Rogus-Pulia, PhD, CCC-SLP on the American Board of Swallowing and Swallowing Disorders (AB-SSD) website within their 2025 Summer Series, titled: “Preserving the Joy of Eating: Rethinking Dysphagia Management in Dementia Care.”
Summary of Prevalence
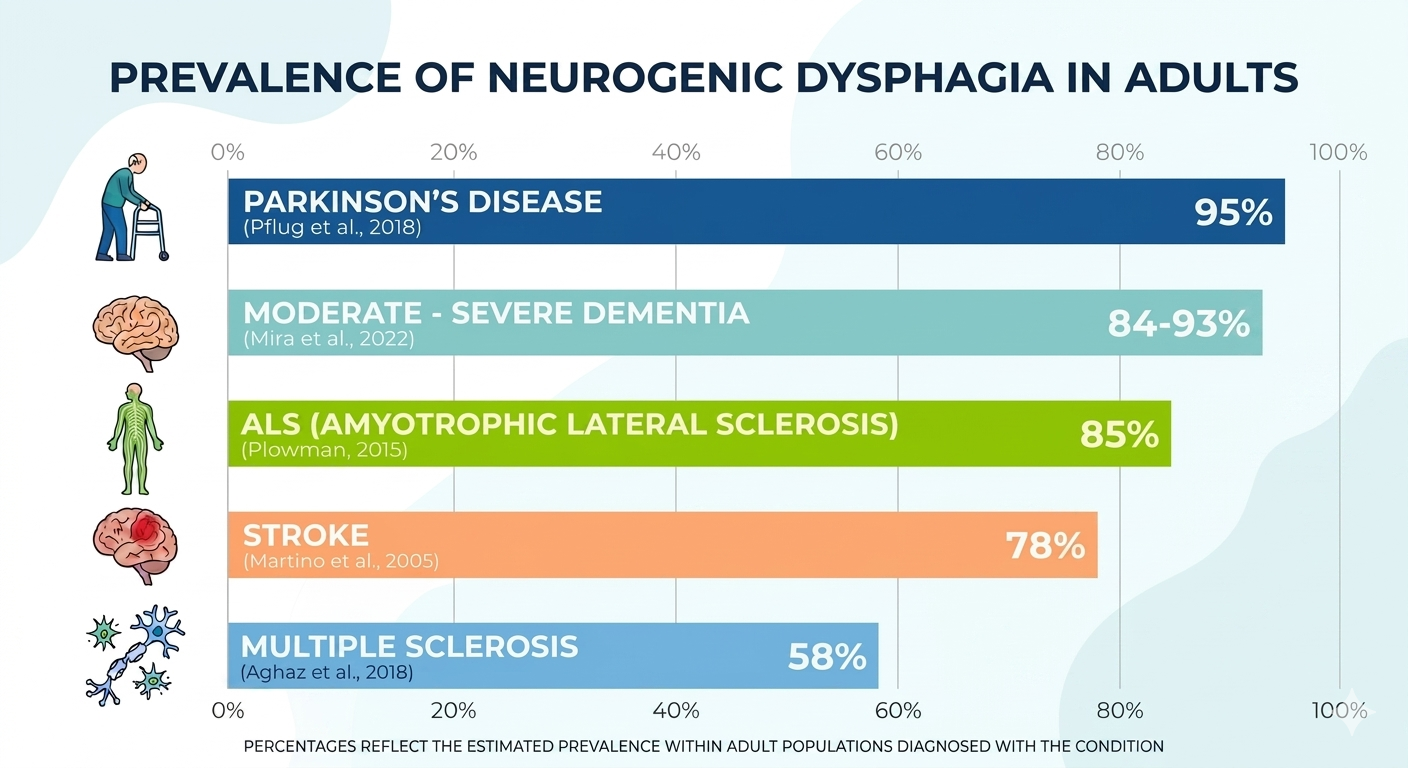
Summary of the Prevalence of neurogenic dysphagia and the need for referrals to speech-language pathologists (SLP) who specialize in dysphagia.
The Hidden Danger: Under-Evaluated!
I have been writing about this issue of “under-diagnosis” of dysphagia in SwallowStudy.com since 2017. It was a major theme at our Dysphagia Research Society meeting that year (see this link). The understanding of this complex process of swallowing is poor among the public and even many healthcare professionals. Maybe one of the issues has been that many anatomy images show a simple tube from the mouth right to the stomach!
Neurogenic dysphagia and all dysphagias are poorly understood due to these poor anatomical images of the swallow. They show the swallow as a simple tube from mouth to stomach! This leaves the public asking: “How could I possibly have trouble swallowing?!”
With this poor awareness of dysphagia, the issue often goes under-reported, under-referred, under-evaluated, and under-treated – even in the neurologically impaired population. Dr. Patel and colleagues (2018) highlighted the significant health and economic burden that dysphagia has on the public in the US healthcare system, especially exacerbated by these delays in care.
See this excerpt from a dysphagia awareness month article, by former DRS president Dr. Nadine Connor, on the Dysphagia Research Society’s website: DysphagiaResearch.org:
“In hospitalized patients, people with dysphagia stay longer, have higher costs, and are more likely to have worse outcomes (Patel et al, 2018). Higher costs contribute to substantial economic and societal burden. Dysphagia is responsible for an estimated $7 billion in additional hospital costs per year (Patel et al, 2018). Despite the extensive impact dysphagia has on health and quality of life, unfortunately, not everyone seeks treatment. In fact, evidence supports that only about 50% of individuals with dysphagia seek treatment (Adkins et al, 2019).” (see references in article)
Sensory vs. Motor Deficits
One of the most misunderstood aspects of neurogenic dysphagia is the role of sensation. Many people assume that the safety and efficiency of the swallow is all about easy movement (motor) of the bolus down a tube. However, as discussed in my Dysphagia Digest article on sensation, we are just starting to understand the importance of sensation on the swallow. For example, the sensory feedback from the internal branch of the superior laryngeal nerve (iSLN) is what tells the brain to cough if food or liquid enters the airway.
When a neurological condition causes “silent aspiration,” the person does not cough when liquid drops to and below the vocal cords into the trachea. They also may not sense when food is getting stuck in the lower throat near the airway. This places them at risk for actual airway obstruction or choking. Some people with neurogenic dysphagia have no idea they are in danger.
This is why a clinical bedside swallow evaluation by the speech pathologist may not be enough. I always tell people that I have not developed my x-ray vision yet! Therefore, we need to see what is happening inside with x-ray or endoscopy.
The “Gold Standard” of Care: Comprehensive Dysphagia Evaluations
Because neurogenic dysphagia is so complex, a medical SLP must have “eyes on the inside.” At SwallowStudy & Associates, we advocate for thorough multiphase dysphagia evaluations that may require instrumental swallowing assessments.
We must know what is happening in the oropharyngeal and pharyngoesophageal stages to adequately plan a targeted treatment. This is:
Why is the dysphagia happening & the What can we do about it?
Knowing why someone is aspirating or has residue is the foundation of any treatment plan, along with what is causing this dysphagia symptom in the first place.
Instrumental Assessments:
- Videofluoroscopic Swallow Study (VFSS/MBSS): A motion X-ray or movie of the swallow from the lips to the lower esophagus or stomach that allows us to see the timing of the brain’s signals and the movement of the bolus in real-time. We analyze the oral phase, pharyngeal phase, and esophageal phase to determine what safety and efficiency issues are present. We may see that food is stuck, but we cannot test for actual *strength* of muscle action. We can only infer when that residue may be a result of weakness or mis-timings or both.
- Fiberoptic Endoscopic Evaluation of Swallowing (FEES): A small camera is passed through the nose to view the anatomy, movement, secretions, airway protection, and the residue left behind after a swallow. Please see this blog for more details on FEES (“The Proof is in the Pudding”).
* Note: To fully test the strength of the squeezing action of the pharynx and esophagus, one would need manometry. See prior blogs summarizing Dysphagia Research Society sessions on High Resolution Manometry (see the 3rd talk discussed in this blog) & High Resolution Pharyngeal Manometry).
Without these tools, we are essentially “guessing” at what the brain is doing. For a patient with a neurological disorder, a guess isn’t good enough.
With that said, there are times when a person is not ready for an instrumental swallowing assessment. Potentially the person is too agitated, too lethargic, or additional testing may not be in line with the person’s goals of care. It is important for these considerations to be discussed thoroughly with the person (and primary caregivers) and documented well in the medical record. Please see this essential article and their algorithm in Figure 1 from Garand and colleagues (2020): “Assessment Across the Life Span: The Clinical Swallow Evaluation.” The algorithm asks the clinician to consider with the person and medical team: Has the Clinical Swallow Evaluation provided adequate information to plan treatment? If the answer is “yes,” and only a bedside clinical swallow evaluation is needed, then maybe the person falls into one of these 4 categories below.
4 Reasons When an Instrumental Swallowing Examination May Not Be Done:
- Functional swallow or returned to baseline and no further evaluation is needed.
- Known history of dysphagia or mild nature of issues that are not suspected to be a new problem or a progression of the disease.
- Need to delay further testing due to inability to participate, behavioral issues (e.g., agitation or combativeness), or significant iatrogenic issues that need to be resolved first (e.g., just received a lot of an antipsychotic medications that need to be cleared from the system – noting half-life of 3+ days at times).
- Goals of care per the person and/or their healthcare proxy indicate that they do not want further testing (e.g., the person may be on the continuum from palliative care approach through comfort care approaches).
Rehabilitation: The Power of Neuroplasticity
The Pillars of Treatment & Neuroplasticity
The most exciting part of treating neurogenic dysphagia is neuroplasticity—the brain’s ability to reorganize itself and form new neural connections. Here is an introduction to neuroplasticity and dysphagia management.
This image shows the pillars of dysphagia therapy and the foundation on which they sit. Especially with neurogenic dysphagia, it is crucial to first figure out why you are having difficulty swallowing. Remember, dysphagia is a symptom of an underlying issue. The speech pathologist who specializes in neurogenic dysphagia works with the person and their whole medical team, collaborating with the neurologist especially. Early identification may resolve some of the underlying issues or symptoms, especially if issues are reversible. There are reversible causes of “dementia” to review with your neurologist.
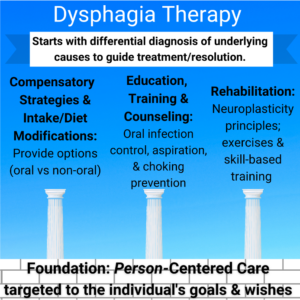
Note: the word “prevention” is used above, but aspiration and choking cannot be prevented 100% of the time. We can try to reduce risks & have risk/benefit conversations in a person-centered approach to treatement.
Details on the 3 Pillars of Dysphagia Management for Neurogenic Dysphagia:
- Compensatory Strategies: Every brain is different. Management must be tailored to the individual’s goals. That is the foundation of person-centered care. Is your goal to enjoy a summer barbeque or your favorite cup of coffee?
- The SLP can provide options and ideas for how to compensate with safer swallowing strategies, which may include changes in how or what you eat and drink and how you take your medications. For example, you can learn maneuvers or strategies to help push down the food and protect your airway better.
- You may find some food and liquid modifications to be helpful.
- All these recommendations are tailored to your wishes, needs, and preferences and in line with your goals of care.
- When considering the types of foods and drinks that you consume, see the info below on the International Dysphagia Diet Standardisation Initiative (IDDSI) below.
- Rehabilitation & Therapeutic Exercise: This is not only strength training, but also skill-based exercise. We don’t just “do exercises”; we use specific protocols and make sure the exercise is targeted to the difficulties seen on the instrumental swallowing assessments. The exercises have to follow the principles of neuroplasticity or neural plasticity, such as use-it-or-loose-it and completing enough repetitions to make a difference. The 10 principles of neural plasticity were integrated into dysphagia treatment by a working group (see Robbins et al., 2008). The exercises not only strengthen, but hope to “re-wire” the brain-to-muscle connections. See this recent article by Krishnamurthy and colleagues (2025) to see the current state of the science in dysphagia-targeted exercises and neuroplasticity.
- Education/Training/Counseling: as the middle pillar notes, the speech pathologist can provide a lot of information on how to reduce risks when possible. Aspiration and choking may not be able to be prevented 100% of the time.
- Training staff and caregivers can help assist a person to eat and drink and meet their nutrition and hydration needs.
- Keeping the mouth very clean with good oral infection control/oral health, for example, can help reduce aspiration pneumonia risks.
- Biofeedback is a key aspect of education & counseling: Using tools like sEMG or even the visual feedback from a modified barium swallow study image or a FEES camera to show the person exactly what their mouth, throat, and esophagus (with x-ray image) are doing.
More on IDDSI:
IDDSI (International Dysphagia Diet Standardisation Initiative) becomes a vital tool for maintaining quality of life. The standardization of dysphagia diets with clear labels and descriptions of foods and liquids through the IDDSI Framework has helped clinicians, healthcare providers, and people with dysphagia finally speak the same language! That helps in our conversations we have with people in our person-centered care approach.
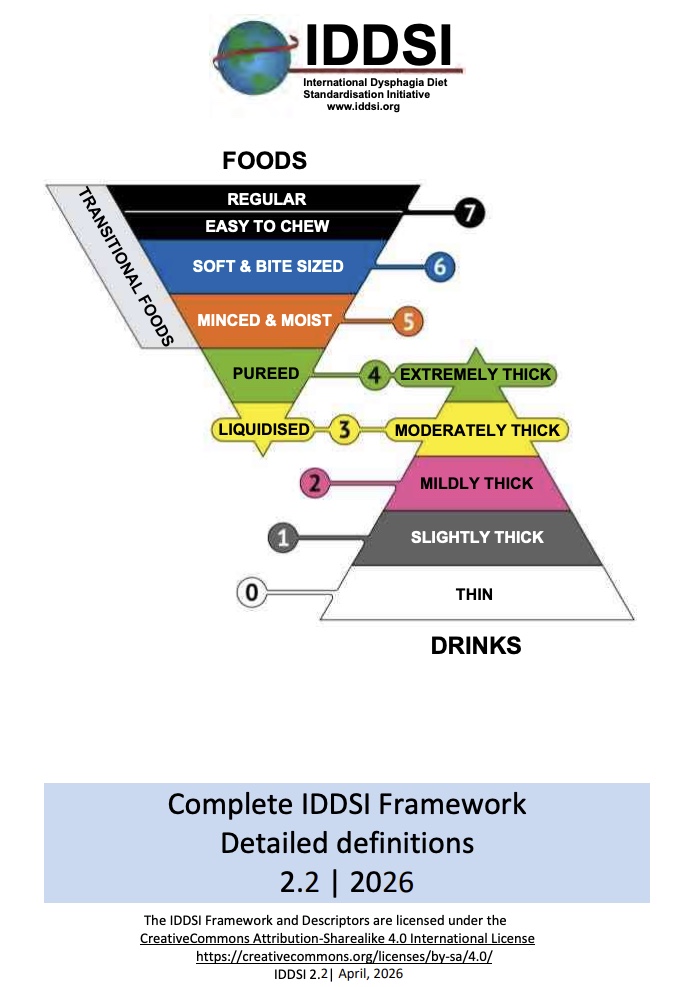
- IDDSI categorizes foods ranging from regular texture to pureed or liquidised foods with clear Testing Methods to determine how hard or difficult a food may be to manage.
- IDDSI categorizes liquids/drinks ranging from thin liquids to extremely thick liquids with a clear IDDSI Flow Test to measure the thickness of the liquids.
Per The IDDSI Framework: “The IDDSI Framework provides a common terminology to describe food textures and drink thickness. IDDSI tests are intended to confirm the flow or textural characteristics of a particular product at the time of testing. Testing should be done on foods and drinks under the intended serving conditions (especially temperature). The clinician has the responsibility to make recommendations for foods or drinks for a particular patient based on their comprehensive clinical assessment.”
There are many resources on SwallowStudy.com regarding IDDSI, as I have been an IDDSI champion since 2014! Please see my 7 IDDSI Updates here, which has links to other articles too. Read more about how IDDSI aides in performing person-centered care in this FAQ section on my website on IDDSI.
Check out this cookbook by Diane Wolfe, with chapters that I authored about dysphagia and IDDSI.
Additionally, in the United States IDDSI Reference Group (USIRG), we have created a person-centered care statement below. This provides an excellent perspective on how IDDSI fosters informed consent and goals of care discussions.
PERSON-CENTERED CARE (PCC) STATEMENT
The IDDSI Framework cannot change, but the diet order can be individualized. Person-centered diet orders specify an individual’s needs within and outside the IDDSI Framework. The medical team works in collaboration with the person’s wishes, preferences, goals of care, and individual abilities. Risks and benefits may be addressed in the informed consent process. Clear orders, communication, and documentation are key to person-centered care.
Conclusion: Awareness Leads to Action
Neurogenic dysphagia is a reminder of how interconnected our bodies truly are. A “swallowing problem” is rarely just about the throat; it may be a window into the health of the nervous system.
As we move through Dysphagia Awareness Month, I encourage you to look beyond the physical act of eating. Dysphagia can impact your quality of life. So many important life events revolve around sharing meals with family and friends. If you or a loved one are experiencing changes in swallowing—especially following a neurological diagnosis—don’t wait to seek help. Reach out to a Board Certified Specialist in Swallowing and Swallowing Disorders (dysphagia) with this find a specialist page. Start the conversation with your medical team now, as you are a key driver of your medical team!
References & Further Reading for Neurogenic Dysphagia
- Aghaz, A., Alidad, A., Hemmati, E., Jadidi, H., & Ghelichi, L. (2018). Prevalence of dysphagia in multiple sclerosis and its related factors: Systematic review and meta-analysis. Iranian journal of neurology, 17(4), 180–188.
- American Speech-Language-Hearing Association (ASHA). Adult Dysphagia. ASHA.org
- Dysphagia Research Society (DRS). Advancing the Science of Swallowing. DysphagiaResearch.org
- Flowers, H.L, Skoretz, S.A., Streiner, D.L., Silver, F.L. & Martino, R. (2011). MRI-based neuroanatomical predictors of dysphagia after acute ischemic stroke: A systematic review and meta-analysis. Cerebrovascular Disease, 32(1), 1-10. doi: 10.1159/000324940
- Garand, K. L. F., McCullough, G., Crary, M., Arvedson, J. C., & Dodrill, P. (2020). Assessment Across the Life Span: The Clinical Swallow Evaluation. American journal of speech-language pathology, 29(2S), 919–933. https://doi.org/10.1044/2020_AJSLP-19-00063 https://pubmed.ncbi.nlm.nih.gov/32650662/
- Gonzalez-Fernandez, M. Kleinman, J.T., Ky, P.K., Palmer, J.B., Hillis, A.E. (2008). Supratentorial regions of acute ischemia associated with clinically important swallowing disorders: A pilot study. Stroke, 39 (11), 3022-8. doi: 10.1161/STROKEAHA.108.518969
- Flowers, H. L., AlHarbi, M. A., Mikulis, D., Silver, F. L., Rochon, E., Streiner, D., & Martino, R. (2017). MRI-Based Neuroanatomical Predictors of Dysphagia, Dysarthria, and Aphasia in Patients with First Acute Ischemic Stroke . Cerebrovascular diseases extra, 7(1), 21–34. https://doi.org/10.1159/000457810
- Huckabee M-L, Lamvik K, Jones R. (2014). Pharyngeal mis-sequencing in dysphagia: Characteristics, rehabilitative response, and etiological speculation. J Neurol Sci., 343, 153–8.
- Im, I., Jun, J. P., Hwang, S., & Ko, M. H. (2018). Swallowing outcomes in patients with subcortical stroke associated with lesions of the caudate nucleus and insula. The Journal of international medical research, 46(9), 3552–3562. https://doi.org/10.1177/0300060518775290
- International Dysphagia Diet Standardisation Initiative (IDDSI). IDDSI.org
- Krishnamurthy, R., Krishnamoorthy, C., Dietsch, A. M., & Natarajan, S. K. (2025). Molecular biomarkers of dysphagia targeted exercise induced neuroplasticity: A review of mechanistic processes and preliminary data on detraining effects. Brain research, 1846, 149287. https://doi.org/10.1016/j.brainres.2024.149287
- Langmore, S. E., Terpenning, M. S., Schork, A., Chen, Y., Murray, J. T., Lopatin, D., & Loesche, W. J. (1998). Predictors of aspiration pneumonia: how important is dysphagia?. Dysphagia, 13(2), 69–81. https://doi.org/10.1007/PL00009559
- Langmore, S. E., Skarupski, K. A., Park, P. S., & Fries, B. E. (2002). Predictors of aspiration pneumonia in nursing home residents. Dysphagia, 17(4), 298–307. https://doi.org/10.1007/s00455-002-0072-5
- Martino, R., Foley, N., Bhogal, S., Diamant, N., Speechley, M., & Teasell, R. (2005). Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke, 36(12), 2756–2763. https://doi.org/10.1161/01.STR.0000190056.76543.eb
- Mira, A., Gonçalves, R., & Rodrigues, I. T. (2022). Dysphagia in Alzheimer’s disease: a systematic review. Dementia & Neuropsychologia, 16(3), 261–269. https://doi.org/10.1590/1980-5764-DN-2021-0073
- Nakao, M., Oshima, F., Maeno, Y. et al. Disruption of the Obligatory Swallowing Sequence in Patients with Wallenberg Syndrome. Dysphagia 34, 673–680 (2019). https://doi.org/10.1007/s00455-018-09970-9
- Patel, D. A., Krishnaswami, S., Steger, E., Conover, E., Vaezi, M. F., Ciucci, M. R., & Francis, D. O. (2018). Economic and survival burden of dysphagia among inpatients in the United States. Diseases of the Esophagus, 31(1), 1-7. DOI: 10.1093/dote/dox131
- Pflug, C., Bihler, M., Emich, K., Niessen, A., Nienstedt, J. C., Flügel, T., Koseki, J. C., Plaetke, R., Hidding, U., Gerloff, C., & Buhmann, C. (2018). Critical Dysphagia is Common in Parkinson Disease and Occurs Even in Early Stages: A Prospective Cohort Study. Dysphagia, 33(1), 41–50. https://doi.org/10.1007/s00455-017-9831-1
- Plowman, E. (2015). Review Article: Is There a Role for Exercise in the Management of Bulbar Dysfunction in Amyotrophic Lateral Sclerosis? Journal of Speech, Language, and Hearing Research, 58, 1151–1166. https://franklinsusanibar.com/wp-content/uploads/2021/05/2015-Plowman-Is-There-a-Role-for-Exercise-in-the.pdf
- Saito, T., Hayashi, K., Nakazawa, H. & Ota, T. (2016). Clinical characteristics and lesions responsible for swallowing hesitation after acute cerebral infarction. Dysphagia, 31, 567-573.
- Sheffler, K. (2024). DRS Digest 2024: Why DRS – section called: Sensation in Swallowing & Airway Protection. Read more here in my SwallowStudy.com blog.
- Reynolds, H., Miller, N., & Walker, R. (2018). Drooling in Parkinson’s Disease: Evidence of a Role for Divided Attention. Dysphagia, 33(6), 809–817. https://doi.org/10.1007/s00455-018-9906-7
- Robison, R., DiBiase, L., Ashley, A., McElheny, K., Anderson, A., Wymer, J. P., & Plowman, E. K. (2022). Swallowing Safety and Efficiency Impairment Profiles in Individuals with Amyotrophic Lateral Sclerosis. Dysphagia, 37(3), 644–654. https://doi.org/10.1007/s00455-021-10315-2
- Robbins, J., Butler, S. G., Daniels, S. K., Diez Gross, R., Langmore, S., Lazarus, C. L., Martin-Harris, B., McCabe, D., Musson, N., & Rosenbek, J. (2008). Swallowing and dysphagia rehabilitation: translating principles of neural plasticity into clinically oriented evidence. Journal of speech, language, and hearing research : JSLHR, 51(1), S276–S300. https://doi.org/10.1044/1092-4388(2008/021)
*******
Thank you for sharing and raising awareness this month!
Do you have questions about the neurological side of swallowing? Leave a comment below or contact us today for more resources. Again, consider finding a board certified specialist in swallowing in your state at this link.
Stay tuned for our next June Dysphagia Awareness Month article, covering esophageal dysphagia, reflux, and that lump in the throat sensation (globus sensation) that has been bothering you!