
Do You Need a Swallow Study for Dysphagia?
by Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Enjoying a good meal with friends and family is something that we may all take for granted. What should we do when something goes wrong with our once fast and well-coordinated swallow function? Read on to find out if you would benefit from a swallow study for dysphagia.
There are many types of swallowing problems or disorders (dysphagia), caused by many different issues. It can be a bit of a puzzle; therefore, it requires different types of evaluations or swallow studies for dysphagia. Please speak with your physician and obtain a referral to a Speech-Language Pathologist.

The goal is to make sure you enjoy a good meal!
How will a Speech-Language Pathologist (SLP) perform a swallow study for dysphagia?
- Clinical Swallowing Evaluation (aka, Bedside Swallowing Evaluation or Dysphagia Examination): These evaluations typically happen at the hospital, rehabilitation facility, and/or skilled nursing facility, but your outpatient SLP could start with a dysphagia evaluation in the clinic. Your SLP will take time to listen to your symptoms and will ask many questions. Try to recall when the problem started and if it started suddenly or gradually. Give your SLP as many details as you can; for example, point to where the food gets stuck, rate any pain associated with swallowing, describe any difficulty you have with food, liquids, and/or pills, and share how your difficulty swallowing (dysphagia) has impacted your life and family.

Do you have difficulty swallowing your pills with liquids? A swallow study for dysphagia should include assessing for pill dysphagia.
Your SLP will also fully examine your mouth, listen to your voice, observe your breathing, and then perform a thorough assessment of how you eat and drink. He/she will observe you swallowing a variety of foods and drinks, comparing different methods of eating and drinking. The SLP will try out strategies to help you eat, drink and swallow as easily and safely as possible. Initial recommendations are given, which may include making appropriate referrals to physicians (i.e., a Neurologist, an Ear Nose and Throat doctor, or a Gastroenterologist). However, the SLP will determine if he/she needs to perform an instrumental examination to further study the swallowing problem. This can help to better define the problem and guide the treatment. We cannot see the structures in your throat. We cannot fully test the function of your swallow once foods and liquids leave your visible tongue. Also, based on a bedside/clinical exam alone, we cannot tell if food, liquid, and/or saliva is getting down the wrong way and into your airway (aspiration). Sometimes aspiration happens silently, without obvious coughing or choking.
One instrumental exam is not necessarily better than another. Depending on the suspected difficulty with your swallow function, the SLP will determine which study to start with (MBSS/VFSS or FEES), as each study has it’s pluses and minuses.
- Two Types of Standard Instrumental swallow studies for dysphagia: These may be performed when you are an inpatient at a hospital or rehabilitation facility, or your doctor may order these directly on an outpatient basis.
1. MODIFIED BARIUM SWALLOW STUDY (also known as the MBSS, the Videoflouroscopic Swallow Study or VFSS)
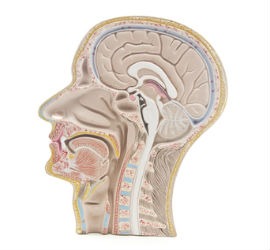
The MBSS/VFSS views swallowing from a side view (like this lateral view) and front/straight-on view (AP view). SLPs analyze this swallow study for dysphagia in a motion x-ray movie, using frame-by-frame analysis to find the underlying structural and physiological problems with the swallow that can be treated with targeted therapy.
You will sit comfortably in a chair within an open x-ray machine in a radiology department or in a mobile van. You will be given different types and quantities of liquids and foods that have been mixed with barium, while the SLP and the radiologist watch your swallowing timing and function. Liquids will be tested via a spoon, cup and straw. The SLP can also give you a barium tablet to evaluate the safest and most efficient way to swallow pills.
This is a motion x-ray of your swallowing. In real-time, they will see the how the structures move to push down the food/liquid and to protect your airway while you are swallowing. They can see how, when, and why food/liquid get into the airway (called penetration or aspiration). They can see if food/liquid remains in your mouth and throat after you swallow (called residue). They can scan down the esophagus to make sure food, liquids and pills do not get hung up in the food tube. If material gets stuck in the esophagus, it could come back up on you and give you problems after the swallow. Scanning the esophagus is done to see if further testing of the esophagus is needed. The SLP will teach you strategies to help you swallow safely and efficiently, and he/she/they can see immediately if these techniques work. Ask the SLP to show you the images too, as a picture speaks a thousand words! The study is recorded and will be analyzed further after you are done.
Advantages of the MBSS/VFSS:
- Test oral, pharyngeal and esophageal phases of the swallow.
- Motion x-ray camera is used with no tube entering your nose.
- Evaluate the speed and range of movement of all the structures as they work together to push the food and liquid out of the mouth, down the throat, and into the esophagus.
- Obtain precise measurements of timing, direction and height in the movements.
- Fully detect when food/liquid squeezes into the airway during the swallow (there is a white-out on the camera during the swallow on a FEES).
2. FIBEROPTIC ENDOSCOPIC EVALUATION OF SWALLOWING (FEES):
You will sit comfortably as you would when you are eating a meal. The SLP can lightly numb your nose to make the exam as comfortable as possible. She will slowly pass a very thin flexible camera (endoscope) through the nose and hold the camera at the top of your throat. You will be able to breathe and talk comfortably the entire time. In a study of 500 examinations, even with no numbing agent in the nose, having a small endoscope in the throat while swallowing was “acceptable” to more than 99% of the patients (Aviv, et.al, 2000). The SLP will be able to see your structures directly and watch how they move when you swallow food and liquid.
Advantages of the FEES over the MBSS:
- Less costly.
- FEES equipment is portable.
- No radiation exposure, so this evaluation can be repeated more readily.
- No barium ingestion, which can cause constipation on a rare occasion.
- Patients can be tested bedside (at hospital, rehab, or skilled nursing facility) or at a doctor’s office without need to be transported to an x-ray department.
- Patients can be observed while eating a typical meal, rather than a specific-limited amount of food and liquid on a MBSS.
- SLP can see if accumulated phlegm, post-nasal drip, secretions, and reflux may be contributing to the problem.
- SLP can see exactly where the food/liquid residue is.
- SLP can directly see the structures and mucous membranes and send pictures to the Ear Nose and Throat doctor. (SLP does not diagnose, but provides a report and recommendations to the Ear Nose and Throat doctor or other physician).
- SLP can perform sensory testing (Fiberotpic Endoscopic Evaluation of Swallowing with Sensory Testing – FEESST), which gives valuable information on your airway protection abilities should something fall towards the airway. The patient’s reaction can be tracked over time to monitor a patient’s progress.
The complex puzzle of swallowing disorders needs us to see inside & collaborate across the team. You are included in this team!
Suggested References on MBSS and FEES/FEESST:
Aviv, J.E. (2000). Prospective, randomized outcome study of Endoscopy versus Modified Barium Swallow in patients with dysphagia. The Laryngoscope, 110 (4), 563-574.
Aviv, J.E., Kaplan, S.T., Thomson, J.E., Spitzer, J., Diamond, B., & Close, L.G. (2000). The safety of Flexible Endoscopic Evaluation of Swallowing with Sensory Testing (FEESST): An analysis of 500 consecutive evaluations. Dysphagia, 15, 39-44.
Chih-Hsiu, W., et al (1997). Evaluation of swallowing safety with Fiberoptic Endoscope: Comparison with Videoflouroscopic technique. The Laryngoscope, 107 (3), 396-401.
Langmore, S.E. & Logemann, J.A. (1991). After the Clinical Bedside Swallowing Examination: What next? American Journal of Speech-Language Pathology, September, 13-20.
Langmore, S.E., Schatz, K., & Olson, N. (1990). Endoscopic and videoflouroscopic evaluations of swallowing and aspiration. Annals of Otology, Rhinology & Laryngology, August, 100, 678-681.