
Dive Into Esophageal Dysphagia: Structure, Motility & More
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Welcome to Week 2 of our National Dysphagia Awareness Month series. This week, we are taking a deep dive down the esophagus (part of the gastrointestinal system). Week 1 was on the neurological system, where we focused on hope for those with neurogenic oropharyngeal dysphagia. Like with the neurological system, we need to explore parts of the gastrointestinal system to fully understand swallowing and swallowing disorders (dysphagia). The esophagus is often overlooked as just a tube from the throat to the stomach. You will learn that it is so much more, and problems caused by esophageal dysphagia can severely disrupt your enjoyment of eating and drinking, as well as your ability to take in enough nutrients, liquids, and medications!
Week 2 will address different types of esophageal dysphagia – with structural & movement/motility issues of the esophagus. Find out how the speech-language pathologist (SLP) can include the esophagus in your comprehensive dysphagia evaluations.
On September 27, 2008, Congress passed a bipartisan statute designating June as National Dysphagia Awareness Month, raising awareness and discussing a condition that affects millions yet remains widely misunderstood. In our article introducing dysphagia awareness month, we mapped out the phases of swallowing, highlighting the complex interactions from mouth to stomach and explaining why we are raising awareness about dysphagia. For an introduction to the esophageal phase, please see this that first blog in this series – under #3 The Esophageal Phase (The Final Stretch). Then come back here for more on esophageal dysphagia!
I have been writing about esophageal dysphagia for years. I am passionate about how much the SLP can contribute to the person’s evaluation and management of their potential esophageal problems. When a person experiences the terrifying sensation of food, liquids, or pills getting stuck, we cannot necessarily divide the issue cleanly: Is it an oropharyngeal problem or an esophageal problem? Swallowing is a continuous, synchronized chain of events with complex throat to esophagus interactions (read more here).
I have written this current blog for the public, as well as for the SLP. (Sorry if it is a bit technical at times, but it would not be a SwallowStudy blog without that!). So, thank you for reading and sharing this broad exploration into:
-
- pharyngoesophageal dysphagia (the junction of the throat to the top of the esophagus),
- esophageal dysphagia, and the
- diagnostic process and technology that help us better define an esophageal dysphagia versus the feeling of something stuck even when maybe nothing is there (called a globus sensation).
Need Dysphagia Specialists for Esophageal Dysphagia
Due to the complexity among the phases of swallowing, a speech-language pathologist (SLP) specializing in swallowing and swallowing disorders is essential. Evaluating the whole swallow – including the esophagus – is within our scope of practice. As an introduction here, consider the following potential issues to sort through:
- Is it a weak pharyngeal pump (pharyngeal squeeze) that has left the esophagus struggling to clear a bolus?
- Is there a bottleneck at the bottom of the esophagus that has caused a backflow and safety issues at the top.
- Is this due to a structural problem of a narrowed esophagus, pouches, and/or a tight lower esophageal sphincter (structural problem)?
- Or, is there a problem with the coordinated squeezing action of the esophagus (motility issue)?
- Is it a referred sensation? This is when something is stuck lower down in the esophagus but the body sends inaccurate messages, making you think the food is stuck in your throat and near your airway. You may fear choking when the issue is actually lower down in the esophagus.
I always say the esophagus is rather dumb! It does not give you good sensory information like your fingertips or face. The sensations, pressures, and pain of esophageal dysphagia can be very scary, but also misleading. You may be restricting what you eat, losing weight, and struggling with meals daily! This highlights the need for a comprehensive swallowing evaluation by an SLP who is evaluating your oral, pharyngeal, pharyngoesophageal, and esophageal phases. The SLP works closely with your medical team, making appropriate referrals to gastroenterology (GI), otolaryngology or ear-nose-throat doctor (ENT), Neurology, registered dietitian nutritionist (RDN), and more.
Anatomy of More Than a Tube
https://training.seer.cancer.gov:ugi:anatomy:esophagus.html
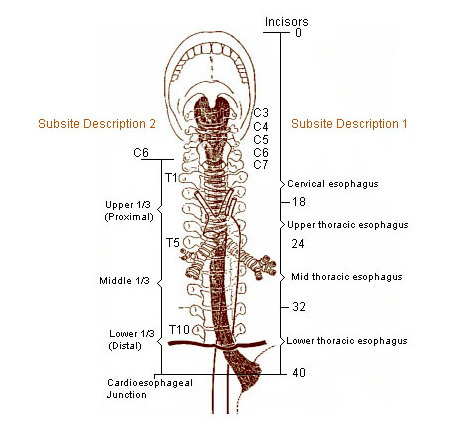
This image shows how we describe the parts of the esophagus:
- Upper ⅓ is the proximal esophagus, with the uppermost section being the cervical esophagus where the cricopharyngeal muscle is at the pharyngoesophageal segment (PES) or upper esophageal sphincter (UES). This portion of the esophagus is striated muscle (aka, skeletal muscle like your biceps). Please see this article for a summary of the cricopharyngeal muscle by Krekeler & Howell (2024).
- Middle ⅓ is sometimes called the mid-thoracic esophagus. This is the transition zone from the striated muscle of the upper esophagus to smooth muscle of the lower esophagus.
- Lower ⅓ is the distal esophagus. This is all smooth muscle and under involuntary or automatic control. You can see in the image above how the esophagus passes through the hole in the diaphragm and joins with the stomach (just under your left breast/chest). People always are shocked at how high up the junction of the esophagus to stomach is.
- Lower Esophageal Sphincter (LES) is not labeled here, but it forms the junction of the esophagus to the stomach (aka, gastroesophageal/GE junction or esophagogastric junction/EGJ – just because everything in medicine needs 2 labels for the same thing, right!?).
- See the numbers along the far right of the image. These are measurements in centimeters. You may see your GI doctor’s endoscopy report saying that you have a stricture (narrowing) in your esophagus at “32 centimeters” from the incisors. That means the stricture is in the lower part of your esophagus. That measurement system allows GI doctors to indicate where the narrowing is.
2 Main Categories of Esophageal Dysphagia
Esophageal dysphagia can be categorized into 2 main categories.
1. Structural Issues
Most of these can be found with endoscopy:
a. Internal:
strictures, rings, webs, diverticulae (e.g., Zenker’s diverticulum), hiatal hernia, esophagitis (e.g., inflammation that can become erosive with chronic reflux), erosions from caustic injury or pill injury from pill impaction, fungal infections, eosinophilic esophagitis, and masses (benign or cancerous).
b. Other:
Surgical changes, like resections and fundoplication can significantly alter the esophagus, as can external compression from masses or enlargement of the heart (cardiomegaly).
2. Motility Issues (esophageal dysmotility)
Cannot be identified by basic endoscopy alone. These require motility studies (manometry) by GI.
Motility problems are hyperfunctioning/spastic OR hypofunctioning/poor squeezing actions. The squeezing action is called peristalsis, and it should progress from top to bottom in primary and secondary clearing waves. Abnormal tertiary (3rd wave) contractions can cause food and liquid to sit or get stuck in the esophagus (aka, esophageal stasis).
Motility problems can also cause the lower esophageal sphincter to not allow food/liquid/pills to pass through to the stomach.
We can categorize these as follows:
a. Primary Motility Problems:
1) Peristalsis problems: esophageal spasms and hypercontractile issues versus hypocontractile or poor contractions, such as ineffective esophageal motility (IEM) or absent contractility.
2) Esophageal Outflow Obstructions: There can be problems with the lower esophageal sphincter (LES) completely relaxing, causing material to not pass easily into the stomach, such as achalasia and other outlet obstructions (EGJOO).
b. Secondary Motility Problems:
1) General muscle wasting and frailty (i.e., sarcopenia) can cause a poor push or squeezing action of the swallow through the pharynx. That sets up a weak peristaltic wave that carries into the esophagus. The striated muscle from the pharynx continues into the top of the esophagus, and those muscles can be greatly affected by generalized weakness.
2) Neurological issues such as MS, Parkinson’s Disease, and Chagas Disease can cause esophageal dysmotility.
3) Autoimmune/connective tissue diseases and systemic diseases, such as Sjogren’s Syndrome, rheumatoid arthritis, lupus, and Scleroderma (which affects the smooth muscle and can cause very severe refluxing).
-
-
- the top ⅓ of the esophagus is striated muscle, so it can be affected by generalized weakness, sarcopenia (muscle wasting), and neurological diseases like Parkinson’s.
- the lower ⅓ is all smooth muscle, so it can be affected by connective tissue diseases.
- the middle ⅓ is the transition zone in the middle of the esophagus where it is common for food to get hung up, called esophageal stasis. High Resolution Manometry (HRM) helps define when this transition zone is too long, causing too much of a gap in the peristaltic wave where the bolus will just stop in the middle of the esophagus.
-
How we define & rate motility problems:
Please see this international review of the most recent Chicago 4.0 classification system for esophageal dysphagia from dysmotility (Fox et al., 2022). This is also a terrific review by Dr. Rena Yadlapati & Dr. Peter Kahrilas, from Northwestern, who many SLPs may recognize for his collaborations with the late Dr. Jeri Logemann.
A word on gastroesophageal reflux disease (GERD). You could think of this as a hypocontractile issue of the lower esophageal sphincter. The LES becomes too relaxed and allows material to come up the esophagus from the stomach. However, GERD does not fit nicely into the Chicago 4.0 classification. Please see this article noting how GERD frequently co-occurs with esophageal dysmotilities.
10 Clinical Clues to Esophageal Dysphagia
While SLPs do not medically diagnose esophageal diseases, they do interview the person with dysphagia, taking exhaustive clinical histories. This provides critical clues to help the doctors perform further differential diagnosis, which is a systematic process of figuring out what is the cause underlying your symptoms of dysphagia.
When conducting the interview – as part of the SLP’s clinical bedside swallowing exam (CBSE) or prior to your outpatient videofluoroscopic swallow study (VFSS, aka MBSS) – listen closely to the person’s answers to these 10 questions. You may hear the 10 warning signs of esophageal dysphagia. These will guide your evaluation, as well as your critical referrals to gastroenterology (GI) and/or Ear, Nose, and Throat (ENT) doctors.
| Clinical Clue Topic | Detailed Questions & Clinical Significance |
| 1. What is getting stuck & when? | Ask: Do just solids, like breads and meats get stuck, or other foods? Do large pills get stuck? Is the problem also with liquids? Does it happen right away or later in the meal?
|
| 2. Where is it stuck? | Ask: Can you point with 1 finger to where the food, liquid, and/or pills feel stuck?
|
| 3. Is there a Globus Sensation (i.e., Lump-in-the-throat sensation) | Ask: Does this feeling of something stuck only happen with swallowing meals and pills, or does it happen all the time?
|
| 4. Stuck sensation clears with Liquid Wash? | Ask: Does a sip of liquid help or cause more problems?
|
| 5. Is there Painful Swallowing (Odynophagia)? | Ask: when the material feels stuck, do you have pain? Rate the pain? Does it radiate to the ears, to the back, or to the throat?
|
| 6. True Regurgitation versus Vomiting? | Ask: Are you feeling nausea and then vomiting? Or, do you eat or drink and then it comes back up on you (regurgitation of undigested food, liquid, pills)? How often? When? What is the material you are spitting out (i.e., stringy sputum, frothy sputum, phlegm tinged with liquids you drank and food particles)?
|
| 7. Bad Breath (Halitosis)? | Ask: Have you or others noticed bad breath? When?
|
| 8. Coughing after the meal (Post-Prandial cough)? | Ask: When do you cough?
|
| 9. Do you get full quickly? (Early Satiety) | Ask: How much food do you eat before you feel full? Do you get full quickly?
|
| 10. Weight Loss? | Ask: Have you had unintentional (not planned) weight loss? Is it related to fear of swallowing and fear of choking? Are you self-limiting your diet?
|
Other Impacts: Quality of Life?
It is important to also evaluate the impact of dysphagia on the person’s quality of life with scales like the EAT-10. This person-reported outcome measure (PROM) has been translated into many languages and is an easy 10 question survey. Some of the questions address quality of life, such as: asking if the swallowing problem has affected the person’s pleasure of eating, if it is causing stress, and if it limits their ability to go out for meals.
In summary, the SLP’s interview needs to ask more than just a basic 10 questions on the EAT-10 scale. The SLP needs to probe deeper to uncover potential esophageal dysphagia issues with the detailed esophageal questions above. Research has found that EAT-10 is not specific enough for detecting esophageal dysphagia (Marvin & Thibeault, 2020). For example, these researchers noted that the question: “When I swallow food sticks in my throat” was only associated with residue in the pharynx, but NOT associated with residue in the esophagus. That makes sense, as Marvin & Thibeault showed how poor our sensation of the location of residue is poor. Let’s talk about that more.
When the Mind Plays Tricks: Faulty Referred Sensations
One of the biggest hurdles in diagnosing esophageal dysphagia is that the esophagus is not wired for precise sensory feedback. The incoming sensory information via the afferent pathways from the Vagus Nerve (Cranial Nerve X) give limited information. Therefore, one has trouble localizing or pointing to exactly where the material is stuck.
Marvin & Thibeault (2020) studied 301 persons who reported sticking sensations (people were excluded if they had any head/neck cancer, muscle disease, or neurological dysphagia). Prior to completing a videofluoroscopic swallow study and an esophagram, the participants were asked to point to all the areas where they felt the food/liquid/pills getting stuck:
A. Throat/pharynx (left, middle, right),
B. Sternal notch or cervical esophagus area, and/or
C. Chest or thoracic esophagus area.
Findings were:
- Only 34% accurately pointed to their problem location!
- 73% of people pointed to the neck in general, meaning A and/or B. (37% just A, 18% A + B, and 18% just B).
- Only 24% (72/301) actually had food getting stuck in the throat/pharynx (pharyngeal dysphagia).
- 78% had actual esophageal findings. The authors noted that 60% of those problems could lead to foods/liquids/pills getting stuck.
- Only 9% pointed to the chest/thoracic esophagus area (C). Another 18% pointed to only B and 6% pointed to B + C.
This is not new information! This sensory inaccuracy was highlighted 20 years ago in research by Smith et al. (1998) regarding people with lower (distal) esophageal mucosal rings who were studied with barium swallow/esophagrams. Among individuals diagnosed with distal rings, only 12 out of 16 felt it when food got stuck in the lower esophagus (food impaction of a marshmallow). Even more alarming, only 19% pointed accurately (localized it) to the mid to lower chest. Out of the 56% of people who felt it and localized it high up in the neck, NONE of those had actual pharyngeal dysphagia or pharyngoesophageal dysphagia.
In summary, a person pointing directly to their Adam’s Apple (larynx) or sternal notch may actually be experiencing a referred sensation from a problem further down in the esophagus. There may be an esophageal stricture, a hiatal hernia, or an esophageal ring (like a Schatzki’s Ring).
If an SLP performs a standard Videofluoroscopic Swallow Study/VFSS (aka, Modified Barium Swallow Study/MBSS) and stops tracking the moment the food/liquid/pills clear the pharynx, they may tell a person “everything looks normal.” But what if a serious structural, motility, or obstructive issue is hiding just inches below. This is why a thorough multi-phase evaluation that scans down the esophagus is crucial.
Modernizing Fluoroscopy: “To Sweep or Not to Sweep”
The standard VFSS/MBSS must be modernized. Some clinicians do not scan the esophagus at all. Others have historically referred to quickly checking the esophagus at the end of a VFSS/MBSS as an “esophageal screen.”
However, as noted by prominent radiologists like Dr. Cheri L. Canon, MD, FACR, this terminology of a “screen” is incorrect. (She spoke at the 2016 Dysphagia Research Society’s Post-Graduate Course – a decade ago – read more here). Dr. Giselle Carnaby, MPH, PhD, FASHA agreed with Canon at the same 2016 Dysphagia Research Society’s Post-Graduate Course. Both Canon and Carnaby noted that by definition: a screen is used to recognize a problem in a non-referred population. Because these persons are already referred for a known swallowing complaint, an esophageal sweep is a formal diagnostic scan.
That was a decade ago, and we are still encouraging clinicians – and often radiologists – to do more thorough evaluations as standard practice. To emphasize that point, please see my 2016 blog: Good dysphagia evaluations guide dysphagia treatment.
Fortunately in 2019, Dr. Joel Richter and colleagues helped SLPs advocate for multiphase videofluoroscopic swallow studies.
“Since swallowing is a multi-phase phenomenon, swallow evaluation should be comprehensive across all phases.” (Watts et al., 2019, p35)
See their Robust Esophageal Sweep Test (REST) protocol (Watts et al., 2019; Watts et al., 2021). As Dr. Joel Richter, MD, FACP, MACG noted in his Dodd’s Donner Lecture at the 2019 Dysphagia Research Society conference:
“If you don’t look, you miss it 100% of the time.”
He reinforced that the esophagus is in the SLP’s scope of practice. If there is any indication that the bolus is not clearing, the SLP would make a referral. The REST protocol does not simply watch a single sip of thin liquid barium clear via gravity, it demands testing:
- Solid Food with 5 cc. barium paste, following the bite (bolus) through the pharynx and to the stomach. (protocol says graham cracker, as that is what is readily available in hospitals***).
- Multiple person-administered and uncontrolled sips (meaning natural and larger-volume) of liquid. They recommended to challenge esophageal transit with highly viscous liquid (E-Z-Paque 70% w/v), but we use the Varibar Barium and the MBSImP does recommend scanning the esophagus with the mildly thick “Nectar Varibar Barium.”
- 13-mm Barium Tablet
*** Please note the gluten free needs of the person. Additionally, if the person’s difficulty is with harder foods like bread, I would advocate for testing with bread, as many graham cracker brands dissolve too easily.
Again, please see the specific references of Watts et al., 2019 and 2021 for details on their protocol and their definitions of normal, anatomic abnormality (structural issue), and dysmotility (motility issue). These items should clear within 1 minute (with liquid wash as needed). The SLP’s report must document findings, results of liquid wash, and all rationales for the swallow strategies recommended. Adequate report information provides enough information across the continuum of care: for your referrals, the next facility or caretakers, and for the people with dysphagia and their loved ones.
Missing Esophageal Dysphagia
Research on MassTex Imaging’s database of almost 10,000 persons (Litwack et al., 2016) revealed that esophageal abnormalities were actually more common than aspiration (47% vs. 35%, respectively). Therefore, when a person complains of difficulty swallowing and the oropharyngeal phase appears normal, one cannot stop there. Watts and colleagues (2019) studied 307 people and found that 80 had esophageal dysphagia per their REST esophageal sweeps. Out of the people with completely normal oropharyngeal swallows, 37 individuals had significant isolated esophageal dysphagia. Similarly Dr. Anna Miles (2015) performed convenience sampling research on 111 people receiving a VFSS. She noted that 68% of those studies showed an esophageal problem. For a third of those, that esophageal dysphagia was their ONLY problem. Literally, these percentages may represent those individuals still reaching out on Reddit’s “r/dysphagia” who have unanswered questions from ill-defined dysphagia!
If you do not scan down, you miss those people entirely. These are individuals who are struggling with swallowing, and they leave their swallow study being told their swallow is normal. They have no further understanding of their problems, no biofeedback, no strategies for mealtimes and taking pills, and no appropriate referrals. That is not only poor person-centered care, but should not our SLP standard of care.
Advanced Diagnostics: High-Resolution Manometry (HRM)
We know that the bedside swallow evaluation is often not enough. (See Garand et al., 2020 where the authors guide clinical judgement as to when further instrumental testing is needed or not based on their algorithm.)
Often the SLP’s instrumental testing is not enough, and the SLP refers back to the medical team who may consider other tests:
- ENT: transnasal flexible fiberoptic laryngoscopy or transnasal esophagoscopy (TNE).
- GI: Upper GI endoscopy (aka, EGD); may add Functional Luminal Imaging Probe (EndoFLIP). pH Impedance Monitoring, Gastric emptying study, or refer for a barium swallow (e.g., timed barium swallow, esophagram, or full upper GI series).
- The medical team may request chest x-rays; neck, chest, and abdominal CTs; MRIs; and more.
Sometimes these other standard tests are also not enough. In order to capture the rapid pressures and muscular strength of a swallow from the pharynx through the LES, healthcare providers turn to High-Resolution Manometry (HRM) and High-Resolution Pharyngeal Manometry (HRPM).
Mapping the Swallow with Heat Maps
Historically, conventional manometry relied on low-resolution line tracings on long sheets of paper. I recall old dysphagia rounds with GI doctors at a VA hospital in the early 2000’s where we used several long conference tables to spread out printouts of esophageal motility patterns. Thank goodness for modern high-resolution manometry (HRM)!
HRM uses an advanced solid-state catheter equipped with 36 circumferential sensors spaced at 1 cm intervals, rather than the 3-5 cm intervals of old catheters. See Gyawali & Kahrilas (2024) for a history of HRM here. The circumferential data from individual sensors is fused mathematically into signals at each point along the catheter. Because some of these sensors can be placed directly within the pharynx (starting up at the nasopharynx), it captures an extraordinary volume of dynamic pressure data. This more accurately shows the muscular strength of the swallow.
Note: the VFSS or FEES cannot test actual “strength.” We have been only inferring “weakness” from the presence of residue. However, it may not be “weakness” at all – there may be timing and coordination issues that have caused the residue (poor efficiency of the swallow).
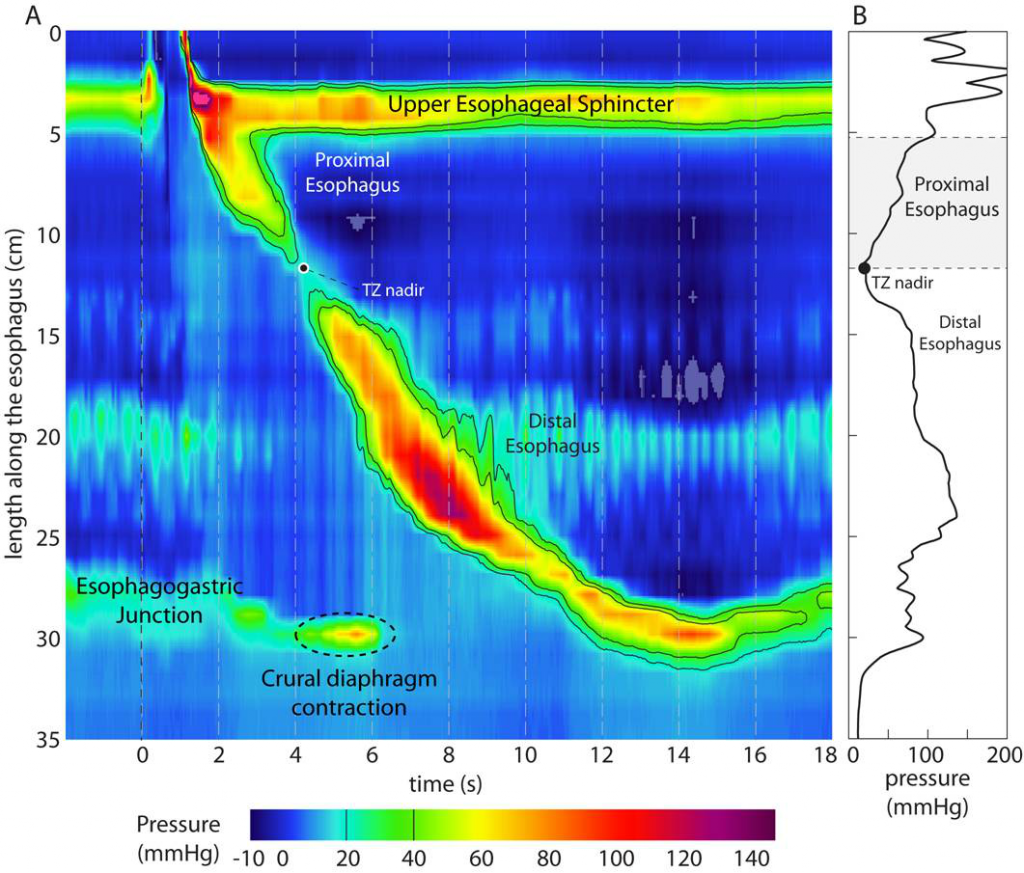
I love the rainbow-colored spatial-temporal “heat maps” that HRM and HPRM generate. The plots have sensor location information top to bottom on the y-axis (nasopharynx to below LES) over time on the x-axis (see image below):
- Bright Red & Warm Colors: Indicate areas of high pressure, which may demonstrate good contractile clearance pressures over time (e.g., the closing of the nasopharynx, the pharyngeal stripping wave, and the esophageal peristaltic wave closing down on the tail of the bolus).
- Cool Blue: Represents open segments of atmospheric pressures or low-pressure relaxation zones.
When tracking a normal swallow, manometry reveals a beautifully timed sequence. This should appear slanted down to the right, as the map progresses over time on the x-axis. The first high-pressure red zone marks nasopharyngeal closure. The bolus then glides through a low-pressure blue zone, followed immediately by a high-pressure red clearing wave at the tail of the bolus.
Esophageal dysphagia and esophageal dysmotility can be tested more thoroughly with high resolution manometry (HRM), showing these pressure or heat maps. HRPM evaluates the pharynx too. HRIM is the addition of impedance testing, showing the presence of bolus in purple to help see when food/liquid is stuck or going back up the esophagus into the throat.
Looking into the “Deep Blue Sea”
While the eye-catching red zones tell us about muscle contraction, the blue zone holds vital clinical data, per Dr. Timothy McCulloch MD, FACS, of University of Wisconsin-Madison’s Division of Otolaryngology/Surgery. See my article from 2015 highlighting exciting research from the 2015 Dysphagia Research Society (DRS) meeting, summarizing Dr. McCulloch’s work in HRM in #3.
The low-pressure transport window is where the bolus actually travels.
“Data is easily lost in the blue sea,” per Dr. McCulloch. This low-pressure zone contains the “real stuff” clinicians worry about, as it dictates whether a bolus is clearing seamlessly, getting stuck, or flowing backward.
To capture what happens inside this blue zone, clinicians utilize High-Resolution Impedance Manometry (HRIM). By adding intraluminal impedance sensors to the catheter, the system measures electrical resistance changes caused by the bolus itself. On the color plot, the bolus is illuminated in a distinct purple color. This allows clinicians to see bolus transit or retrograde flow (backflow) live, mapping out exactly how safely and efficiently material moves down the pharynx and esophagus without relying entirely on continuous radiation as the VFSS does.
I cannot possibly share enough about HRM here. Learn more. Begin with the early use of HRM:
- Learn more about the history of clinical implementation of manometry in speech pathology via Knigge, M.A, Thibeault, S. & McCulloch, T.M. (2014) in the journal Dysphagia.
- Read about automated pharyngeal pressure data analysis in Mielens, J.D., Hoffman, M.R., Ciucci, M.R., Jiang, J.J. & McCulloch, T.M. (2011).
- See High Resolution Manometry webinar on NFOSD by Molly Knigge, MS, CCC-SLP, BCS-S.
- Explore more training webinars and resources on complex swallowing disorders at the National Foundation of Swallowing Disorders (NFOSD).
AI Assistance for HRM
The future of dysphagia diagnostics is arriving rapidly through machine learning, specifically artificial neural networks (ANN). According to Dr. Timothy McCulloch’s DRS session in 2015, the last 10 years have been full of research to use their automated data extraction (via MATLAB) to train an artificial neural network (ANN), which is a type of AI. Many researchers have been teaching computers to recognize these specific multi-dimensional pressure signatures or swallow patterns. See early work in pattern recognition for people with Parkinson’s Disease (Jones et al., 2018). This will allow computers to predict if a swallow pattern is normal or abnormal with well over 90% accuracy, especially when HRPM is paired with VFSS or FEES.
HRM Shows How Pharyngeal Swallow Strategies Affect Esophageal Clearance
One of the most fascinating reasons to prioritize multiphase dysphagia evaluations is that our pharyngeal treatments and strategies do not exist in a vacuum. Specific swallow strategies thought to be helpful for pharyngeal clearance can actually disrupt esophageal peristalsis.
Consider the common swallow strategy of “double swallow” to clear stubborn food left over in the throat (pharyngeal residue). High-Resolution Manometry (HRM) has revealed that if a second swallow is initiated within 10 seconds of the primary swallow, it can inhibit the secondary peristaltic clearing wave in the esophagus (per Dr. Ashli O’Rourke at ASHA, 2014). This secondary wave is a crucial automatic cleaning wave triggered by the physical distension of the esophagus itself.
When an SLP instructs a person to double swallow rapidly, they may clear the throat at the direct expense of freezing the esophagus. This could lead to more significant food residue (stasis), discomfort/pain, and even increase the risk for retrograde flow back up into the airway. Therefore, the SLP needs to maintain a holistic view from the mouth to the stomach.
I have frequently seen people who are fearful of choking – often due to the referred sensation from esophageal dysphagia or a globus sensation. They may change their pattern of eating to the overly cautious strategy of piecemeal swallowing (this is swallowing 2-3 times just to get one small bite out of the mouth). The person may think that is “safer.” In reality, they are causing even more disruption to their esophageal clearance. The esophagus performs better when you give it a good bolus size and swallow once (after chewing appropriately to make the food “swallow ready”). We use the video screen as biofeedback during a VFSS to show the person in real-time that their confident swallow of the entire chewed bolus travels much more effectively through the esophagus, reducing the esophageal stasis!
Fortunately esophageal motility testing, like the HRM, has shown us the impact of our swallowing strategies. An effortful swallow seems to help esophageal clearance and a Mendelsohn Maneuver both help in the pharyngoesophageal phase, allowing for better opening of the upper esophageal sphincter. However, the Mendelsohn Maneuver may negatively impact esophageal clearance at times (Hoffman et al., 2012; Doeltgen et al., 2017; Nekl et al., 2016).
As clinicians, we are often balancing our recommendations against potential risks. We cannot offer safe and informed options if our visual field stops at the cricopharyngeal muscle and does not scan the esophagus with solids, liquids and pills.
Broadening Your Dysphagia Toolbox for Esophageal Dysphagia
To the Public: I hope this article has given you tools to advocate for yourself or a loved one.
To Healthcare Providers: In dysphagia evaluation and management, we cannot look at every person with the same old lens or with a one-size-fits-all approach. We must continuously and critically analyze our protocols. Ask yourself: What else? Am I looking at the whole swallow – from the lips to the stomach? SLPs need to understand the complex physiological relationships between the pharynx and the esophagus. Comprehensive evaluations lead to prompt referrals and targeted treatments.
SLPs and the public need to advocate for multi-phase videofluoroscopic swallow studies. These can be considered oroesophagrams, as my dysphagia professor Dr. Joanne Robbins used to say in the 1990s, showing this lips to stomach idea is not a new one! Then, when the SLP’s instrumental swallowing evaluations are not enough, the SLP refers to the GI, ENT, and other members of the person’s medical team. People can request more objective and advanced diagnostics like HRM/HRIM and HRPM and when the standard imaging leaves questions unanswered. This advocacy can ensure that people receive the most accurate path to differential diagnosis and eventually dysphagia management and rehabilitation.
******
thank you for reading & sharing!
Stay tuned for Week 3 of our Dysphagia Awareness Month series, where we will navigate the profound structural challenges of Cancer and Survivorship, including Radiation-Associated Dysphagia (RAD).
******
For more information on how to navigate dysphagia evaluations and to understand your dysphagia, please see my chapter in the cookbook: Cooking for Dysphagia. I have recommendations on how to manage your dysphagia, safer swallow strategies, tips for holidays and traveling, and food/liquid modification options (IDDSI.org), and more. Please see this article about the cookbook by Diane Wolff in Mayo Clinic Press.
Cooking for Dysphagia and other Swallowing Problems: 101 Delicious Recipes and Techniques for Safer, Easy Eating
References for Esophageal Dysphagia:
Belafsky, P. C., Mouadeb, D. A., Rees, C. J., Pryor, J. C., Postma, G. N., Allen, J., & Leonard, R. J. (2008). Validity and reliability of the Eating Assessment Tool (EAT-10). The Annals of otology, rhinology, and laryngology, 117(12), 919–924. https://doi.org/10.1177/000348940811701210
Canon, D. (2016, February). Dysphagia: Misused and Misunderstood, A Radiologist’s Perspective. Session presented at the Post-Graduate Course at the Dysphagia Research Society 24th Annual Meeting, Tucson, AZ.
Carnaby, G. (2016, February). Promoting Evidence and Standards in Clinical Assessment. Session presented at the Post-Graduate Course at the Dysphagia Research Society 24th Annual Meeting, Tucson, AZ.
Doeltgen, S. H., Ong, E., Scholten, I., Cock, C., & Omari, T. (2017). Biomechanical Quantification of Mendelsohn Maneuver and Effortful Swallowing on Pharyngoesophageal Function. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery, 157(5), 816–823. https://doi.org/10.1177/0194599817708173
Fox, M. R., Sweis, R., Yadlapati, R., Pandolfino, J., Hani, A., Defilippi, C., Jan, T., & Rommel, N. (2021). Chicago classification version 4.0© technical review: Update on standard high-resolution manometry protocol for the assessment of esophageal motility. Neurogastroenterology and motility, 33(4), e14120. https://doi.org/10.1111/nmo.14120
Garand, K. L. F., McCullough, G., Crary, M., Arvedson, J. C., & Dodrill, P. (2020). Assessment Across the Life Span: The Clinical Swallow Evaluation. American journal of speech-language pathology, 29(2S), 919–933. https://doi.org/10.1044/2020_AJSLP-19-00063
Gyawali, C. P., & Kahrilas, P. J. (2023). A Short History of High-Resolution Esophageal Manometry. Dysphagia, 38(2), 586–595. https://doi.org/10.1007/s00455-021-10372-7
Hoffman, M. R., Mielens, J. D., Ciucci, M. R., Jones, C. A., Jiang, J. J., & McCulloch, T. M. (2012). High-resolution manometry of pharyngeal swallow pressure events associated with effortful swallow and the Mendelsohn maneuver. Dysphagia, 27(3), 418–426. https://doi.org/10.1007/s00455-011-9385-6
Jones, C. A., Hoffman, M. R., Lin, L., Abdelhalim, S., Jiang, J. J., & McCulloch, T. M. (2018). Identification of swallowing disorders in early and mid-stage Parkinson’s disease using pattern recognition of pharyngeal high-resolution manometry data. Neurogastroenterology and motility, 30(4), e13236. https://doi.org/10.1111/nmo.13236
Kang, C. H., Hentz, J. G., & Lott, D. G. (2016). Muscle Tension Dysphagia: Symptomology and Theoretical Framework. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery, 155(5), 837–842. https://doi.org/10.1177/0194599816657013
Kang, C. H., Zhang, N., & Lott, D. G. (2021). Muscle Tension Dysphagia: Contributing Factors and Treatment Efficacy. The Annals of otology, rhinology, and laryngology, 130(7), 674–681. https://doi.org/10.1177/0003489420966339
Krekeler, B. N., & Howell, R. J. (2024). Cricopharyngeus muscle dysfunction: a poorly defined disorder from diagnosis to treatment. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS): affiliated with the German Society for Oto-Rhino-Laryngology – Head and Neck Surgery, 281(9), 4519–4527. https://doi.org/10.1007/s00405-024-08644-7
Litwack, A., Arsenault, J.K., Brand, S., Morgan, L. & Baumer, J. (2016, March). Prevalence of esophageal findings in adults via MBS with esophageal assessment. Poster presented at the Dysphagia Research Society Annual Meeting, Tucson, AZ.
Marvin, S., & Thibeault, S. (2020). Pharyngeal Versus Esophageal Stasis: Accuracy of Symptom Localization. American journal of speech-language pathology, 29(2), 664–672. https://doi.org/10.1044/2019_AJSLP-19-00161; https://pubmed.ncbi.nlm.nih.gov/32142366/
Miles, A., McMillan, J., Ward, K. & Allen, J. (2015). Esophageal visualization as an adjunct to the videofluoroscopic study of swallowing. Otolaryngol Head Neck Surg, 152(3), 488-93. https://www.ncbi.nlm.nih.gov/pubmed/25605697
Nekl, C. G., Lintzenich, C. R., Leng, X., Lever, T., & Butler, S. G. (2012). Effects of effortful swallow on esophageal function in healthy adults. Neurogastroenterology and motility, 24(3), 252–e108. https://doi.org/10.1111/j.1365-2982.2011.01864.x
de Padua, F., Herbella, F. A. M., & Patti, M. G. (2022). The prevalence of gastroesophageal reflux disease in named manometric patterns of dysmotility according to the Chicago Classification 4.0. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus, 35(10), doac023. https://doi.org/10.1093/dote/doac023
Smith, D. F., Ott, D. J., Gelfand, D. W., & Chen, M. Y. (1998). Lower esophageal mucosal ring: correlation of referred symptoms with radiographic findings using a marshmallow bolus. AJR. American journal of roentgenology, 171(5), 1361–1365. https://doi.org/10.2214/ajr.171.5.9798879; https://pubmed.ncbi.nlm.nih.gov/9798879/
Watts, S., Gaziano, J., Jacobs, J. & Richter, J. (2019). Improving the diagnostic capability of the modified barium swallow study through standardization of an esophageal sweep protocol. Dysphagia, 34(1), 34-42. https://www.ncbi.nlm.nih.gov/pubmed/30635777
Watts, S., Gaziano, J., Kumar, A., & Richter, J. (2021). Diagnostic accuracy of an esophageal screening protocol interpreted by the speech-language pathologist. Dysphagia, 36(6), 1063–1071.
Yadlapati, R., & Kahrilas, P. J. (2021). How Updates in Chicago Classification Impact Clinical Practice. Foregut (Thousand Oaks, Calif.), 1(3), 207–215. https://doi.org/10.1177/26345161211039851