
Transform Dysphagia Care: Thrive with 8 Tips on Person-Centered Care
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction to Person-Centered Care
If you or a loved one has recently been diagnosed with a swallowing disorder (dysphagia), the first thing you need to know is: You are not alone. Person-centered care can help make sure this is not the end of your relationship with good food and drink. What does living with dysphagia involve for you:
- collaborating with your medical team to maintain abilities;
- strengthening and improving your swallow;
- learning new strategies for mealtime success; and
- adapting and compensating as needed?
Dysphagia evaluation and therapy is not just about restrictions in what you eat and drink. Dysphagia management must prioritize Person-Centered Care (PCC). This approach shifts the focus away from rigid orders of a doctor telling a patient what to do. Instead, we shift to seeing the person — as more than a “patient” — and as the driver of their own medical team. PCC considers the person’s unique life goals, wishes, preferences, and quality of life at the center of clinical decision-making.
For June’s Dysphagia Awareness Month, our blog series offered three key windows into this dysphagia world to prepare you and your caregivers to start to become your own advocates:
- Neurogenic Dysphagia: Exploring how neurological conditions like a Stroke or Parkinson’s Disease can affect the safety and efficiency of swallowing in sudden or gradual ways, and sometimes people with these issues cannot feel liquid getting down the wrong way or sense that food is getting stuck.
- Esophageal Dysphagia: Investigating structural and motility issues within the food tube to the stomach, the esophagus.
- Head and Neck Cancer-Related Dysphagia: Navigating the complex swallowing changes caused by tumors, surgeries, and chemoradiation treatments.
Find Underlying Causes of Dysphagia: First Step in a Person-Centered Care Approach
While these three areas are highly common, dysphagia can also stem from many other underlying causes. It is important to have comprehensive evaluations, as finding the underlying causes of your difficulty swallowing is a foundation of thorough person-centered care and the start of your treatment. Remember, dysphagia is not a disease in-and-of-itself. Dysphagia is a symptom.
We have to constantly ask: what are we missing, what else, what is causing this?
Often there may be multiple underlying issues in one person. We call that “multifactorial.” In other words, one issue may exacerbate another.
Here is an introduction to some of these other potential issues:
- Age-related muscle loss and weakness (presbyphagia or also called sarcopenia). Follow work in the field of dysphagia by Dr. Sonja Molfenter for her work on sarcopenia and frailty, such as Molfenter and team (2015), showing that the throat or pharyngeal muscles can be affected by this loss of “muscle bulk and strength.”
- Generalized weakness, from prolonged hospitalization for example, can cause difficulty swallowing in an already frail individual.
- Spinal surgeries: This is a completely different type of dysphagia that may be caused by spinal surgeries to the neck, such as an ACDF (anterior cervical discectomy and fusion). When the surgery location involves the cervical vertebra from C1 through C7, and the approach to reach the spine is opening up the front of the neck and pushing aside the swallowing structures, it makes sense that this will cause significant difficulty swallowing after the operation. Dysphagia is common often for 1 month or more due to swelling and difficulty clearing residue through the throat and into the esophagus. See Dr. Molfenter’s works also on ACDF: 2023 scoping review and her team’s work first authored by Jones-Rastelli et al., 2025, comparing videofluoroscopic swallow studies to the person-reported outcome measures (PROMs).
- Other underlying causes for dysphagia may be due to severe respiratory illnesses (like COPD), medication side-effects, structural anomalies/abnormalities, severe psychological conditions, and more.
Understanding your pattern of underlying causes allows you and your multidisciplinary teams to advocate for better, more comprehensive and compassionate care.
8 Person-Centered Care Principles & Tools
- Request Person-Centered Care
- Advocate for The IDDSI Framework
- Seek Comprehensive Dysphagia Evaluations
- Start Targeted Dysphagia Therapy with Evidence-Based Practice
- Focus on Oral Infection Control
- Get Creative in the Kitchen
- Learn Tips for Safer Swallowing
- Advocate for Person-Centered Care for All
1. Request Person-Centered Care
Healthcare professionals must remember that the person is the most important member of the medical team. I like to describe this as the person is the driver of their medical team. Person-centered care means that your individual goals matter.
For example, if your goal is to be able to enjoy a glass of champagne at your daughter’s wedding, your dysphagia therapy with a speech-language pathologist (SLP) who specializes in dysphagia should work with you to find a safer way to make that happen. SLPs are moving away from dictating one recommendation option only in their evaluations (e.g., you need to stay strictly NPO). That strict recommendation may have made the SLP feel better, providing what they thought was the safest option. However, there is no perfect-safest option. There are only the person’s informed decisions.
Now, SLPs are moving toward finding out what fits with the person’s goals. SLPs offer a range of options along a continuum of curative through more palliative and comfort-focused approaches. See the two ends of the continuum here:
| A curative or aggressive approach tries to reduce risks of aspiration, choking, and aspiration pneumonia. (Note: there is no perfect solution or safest option that reduces risks 100% of the time) |
↔ |
A palliative care or even comfort care approach focuses on the person’s goals, preferences, wishes, and overall comfort and quality of life – rather than trying to reduce risks at all costs. |
With this person-centered care focus, your team will provide ongoing education you to foster informed decision-making throughout the process. Clinical decisions must align with your personal choices and specific goals of care. See the 3-circles below of evidence-based practice: 1) Current evidence from research, 2) clinical expertise of the team members involved and reaching out to other experts for unanswered questions, and 3) the person’s own perspective and goals of care. This helps the medical team educate the person and necessary caregivers (i.e., the person’s healthcare proxy). This fosters the informed decision-making process.
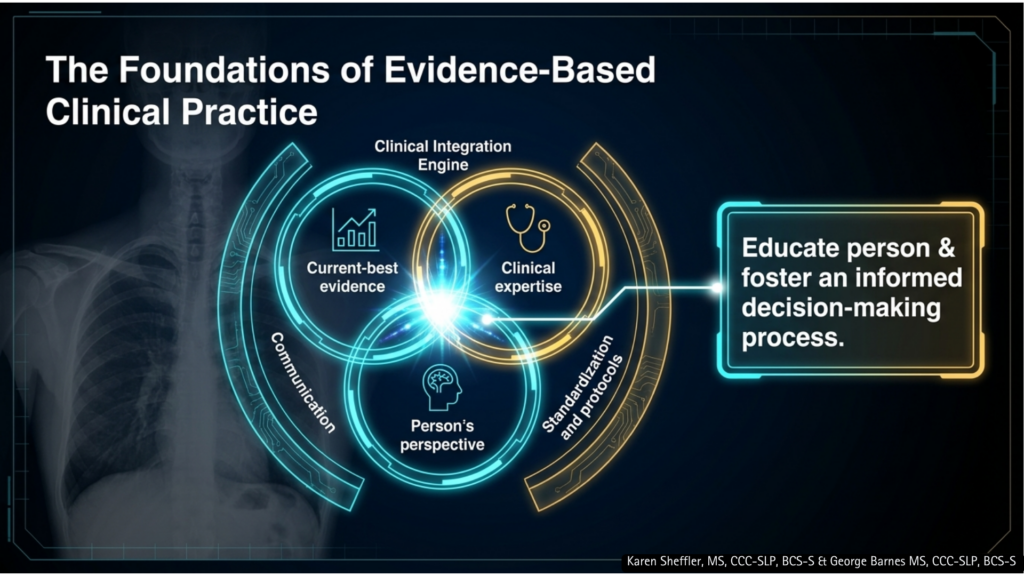
This is the clinical “engine” that the SLP uses to craft a targeted dysphagia therapy program. See how this engine is supported by good communication and standardized protocols/guidelines/policies. What is missing here is reminding the team that thorough documentation of details is important!
Want to Learn More?
- For SLPs and other healthcare providers: hear more about how this person-centered care clinical engine operates on foundations of good communication, standards, and thorough documentation, please see my Medbridge talk with Dr. Yvette McCoy here, called: “Reframing Dysphagia Documentation with a Person-Centered Approach.”
- For patient advocates & law firms: please contact SwallowStudy & Associates, LLC for George Barnes, MS, CCC-SLP, BCS-S and Karen Sheffler, MS, CCC-SLP, BCS-S to provide further webinars & discussions on how these standards affect risk management and litigation. Read more about our expert witness services here.
2. Advocate for The IDDSI Framework (A Common Language, Not a Mandate)
The world of “soft” foods or “thickened” liquids used to be the “wild west,” as everyone had a different labels for dysphagia diets and no one was using the same definitions or descriptions. That was incredibly unsafe! Today, we utilize the International Dysphagia Diet Standardisation Initiative (IDDSI) Framework.
With IDDSI, we are finally speaking the same language — whether you are a person with dysphagia or a healthcare provider across the continuum of care. IDDSI uses standardized labels, descriptions, kitchen tools and guidelines, and testing methods (see Framework and Testing Methods document links in many languages here). Healthcare providers (such as registered dietitians and speech-language pathologists) are champions of the IDDSI implementation and IDDSI adoption within each facility. As a person with dysphagia, if you see that your facility is not using this international standard, you too can ask and advocate for IDDSI!
We want to make sure that when we say “soft” that we know what “soft” means. No more vague and very outdated labels such as“mechanical soft.” What does that even mean?
We want to ensure that when a food is cut-up for safety, that this “bite-size” really follows research on what particle sizes may fall through an airway, rather than block an airway or choke a person.
That is IDDSI.
Understanding IDDSI in Practice
- Evidence-Based Standard: IDDSI is not legally mandatory, but it stands as the only professionally supported and evidence-based standard of practice across the nation and around the world.
- Not Prescriptive: IDDSI is not a rigid mandate. It does not dictate a set of restrictions on what a person is “allowed” or “not allowed” to eat.
- Collaborative Planning: SLPs, Registered Dietitians (RDs), and other healthcare professionals work together alongside the person to meet their specific preferences and care goals.
- Custom Exceptions: Teams can create agreed-upon exceptions to the IDDSI Framework. The IDDSI Framework does not change, but exceptions can be written in a person’s order from the doctor. For example, a person might successfully utilize a Soft & Bite-Sized, Level 6 diet, but have selected breads per the person’s requests and the clinician’s assessments.
- Exception example: if a person loves their toast in the morning, the clinician may give recommendations to help manage the person’s dry mouth before the meal and then to dunk the toast in the coffee to make it more moist and slippery.
- Good documentation is needed regarding these person-centered care requests, rationales, exceptions, and actions.
- See this FAQ on “Exceptions: Bread & Mixed Consistencies” from the USIRG.
- See the United States IDDSI Reference Group’s (USIRG) chart of US-specific resources here.
- IDDSI is a Clinical Tool: Diet modification is merely one tool in our comprehensive dysphagia therapy toolbox. IDDSI does not tell clinicians when to order a modified diet or thickened liquids. Thorough diagnostic testing and critical thinking remain paramount.
- Simple Testing Methods: You can perform simple tests with tools in a kitchen (i.e., fork and spoon tests here in North America or finger or chopstick tests in other parts of the world). IDDSI provides the global kitchen with simple testing methods to evaluate each food and liquid and see what IDDSI Level it falls within.
USIRG’s IDDSI Person-Centered Care (PCC) Statement
The United States IDDSI Reference Group (USIRG) emphasizes this balance through their official Person-Centered Care Statement:
The IDDSI Framework cannot change, but the diet order can be individualized. Person-centered diet orders specify an individual’s needs within and outside the IDDSI Framework. The medical team works in collaboration with the person’s wishes, preferences, goals of care, and individual abilities. Risks and benefits may be addressed in the informed consent process. Clear orders, communication, and documentation are key to person-centered care.
Ultimately, IDDSI provides a universal language across all age groups, cultures, and care settings, making the informed-consent process clearer for everyone involved. Imagine these complex goals of care conversations made a bit easier when we are all using the same terms and descriptions of these Levels of foods and liquids. For example, we use standard labels with 2 identifiers (e.g., Pureed, Level 4 or Mildly Thick, Level 2). This avoids the diet label confusions, and gives clear recommendations to the next level of care. Please see my writing on IDDSI that has spanned from 2014 to 2026 with this example of 7 IDDSI Updates, which has links to prior articles.
3. Seek Comprehensive Dysphagia Evaluations
We have talked a lot about comprehensive dysphagia evaluations during Dysphagia Awareness Month. To reiterate: You wouldn’t let an orthopedic doctor set a broken bone without an x-ray. You would not start treating a lung issue without an x-ray or chest CT. The same exact logic applies to the swallowing function.
While a clinical bedside swallowing evaluation provides excellent initial clues to start digging deeper (like in these pneumonia blogs), we need to advocate for seeing exactly what is happening in the throat.
When the instrumental is needed to guide person-centered care, it may require:
- VFSS (Videofluoroscopic Swallow Study): A moving, real-time x-ray that tracks your swallow mechanics.
- FEES (Fiberoptic Endoscopic Evaluation of Swallowing): A tiny, flexible camera passed gently through the nose to view the throat from directly above.
These diagnostic tests are not designed to “pass” or “fail” a person. Instead, they identify what are the underlying problems with your swallowing and what we can do about them. It may identify which specific postures, maneuvers, and/or food and liquid texture changes can be used to improve your safety and efficiency of getting foods, liquids and pills down to maintain your nutrition and hydration. These instrumental swallow studies will also help target your dysphagia therapy to your needs.
4. Start Targeted Dysphagia Therapy: The Multi-Pillar Framework
Diet modification (i.e., to softer textures or thickened liquids according to IDDSI Framework and descriptors) is often a temporary measure during acute illness or used as a supportive safety net to get over a pneumonia or through a challenging time in your rehabilitative process. Person-centered dysphagia management relies also on targeted dysphagia therapy, which applies specific modalities to the right person at the right time. See these 3 pillars of dysphagia therapy below.
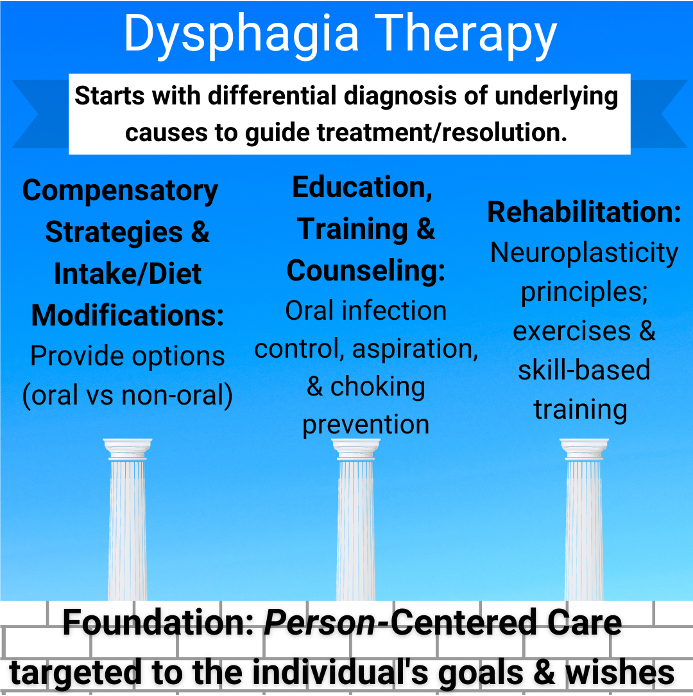
This is a good summary of person-centered care in dysphagia management. It starts with good differential diagnosis. Then these 3 pillars of dysphagia therapy sit on the foundation of the person’s goals and wishes.
By balancing these therapeutic pillars, your clinician helps you target recovery — when possible — rather than relying solely on permanent restrictions.
5. Focus on Oral Infection Control
This is one of the most critical “hidden” secrets of dysphagia management: A clean mouth is a safer mouth.
Every human aspirates micro-amounts of their own saliva during sleep. If your mouth contains high levels of harmful bacteria, that aspirated saliva can travel further down into the lungs and cause aspiration pneumonia. Those harmful bacteria in the mouth may also be aspirated along with the liquid and food particles that are aspirated during your meals or after.
Rigorous oral hygiene—brushing, flossing, rinsing, and keeping tongue, gums, cheeks, lips, and palate clean—is your number one defensive tool for reducing aspiration pneumonia risks and fighting off systemic illnesses.
Please see these other articles on SwallowStudy.com on Oral Infection Control & Oral Health:
10 Trillion Microorganisms vs Your Toothbrush (Part I: Oral Hygiene)
What Do Volcanoes & Mouths Have in Common? (Part II: Oral Microbiome & Saliva)
Take a Trip to the Lungs with 12 Bacterial Species (Part III: Oral Hygiene)
6. Get Creative in the Kitchen
Modified-texture food does not have to be bland, unappealing, or depressing. Keeping the “joy” in every single bite is vital to maintaining nutrition and mental well-being. Check out these top two cookbooks.
Cooking for Dysphagia Cookbook
Learn from Diane Wolff in Cooking for Dysphagia. She cooked years for her mother while she struggled with dysphagia from dementia. Wolff’s cookbook will help you transform your kitchen into a dysphagia-ready kitchen. She believes: “life is too short to eat boring, tasteless food,” (page 11 of cookbook).
This cookbook serves as a testament that you can prepare 101 delicious, safe recipes that look, smell, and taste like “real” food. You will learn how to save time with the “batch cooking method.” From rich, savory sauces to nutrient-dense purees, texture modification can be a culinary art form that you can learn. See also my chapters on: You Have Dysphagia: What’s Next and further help to understand IDDSI.
(Disclosure: I was paid to write these cookbook sections).
Modern Dysphagia Cooking Cookbook
My colleague and friend, John Holahan, BS, MBA created this Modern Dysphagia Cooking guide to “turning family favoriets into dysphagia-friendly dishes.” See Holahan’s article on SwallowStudy.com describing his process of writing this cookbook with co-authors: Laurie Berger, MBA, RD, LD, Paul Haefner, and Nancy A. Yezzi, RDN, LD.
7. Learn Tips for Safer Swallowing at Home (or when in a facility)
Managing dysphagia at home can feel overwhelming, especially during busy seasons or large family gatherings, but these strategies can help foster safer and more comfortable eating:
- Eat Mindfully: Slow down sufficiently to chew and swallow each bite completely before taking the next. Try not to talk with food in your mouth. I know, I am one to talk – I have the gift of gab too!
- Optimize Posture: Ensure an upright, well-supported sitting position during meals. Or, use the positioning recommended based on your comprehensive swallowing evaluation. Prioritize self-feeding whenever possible, as it is naturally safer than being dependently fed.
- Lubricate the Pipe: Ensure the mouth is clean and moist before eating. If dealing with dry mouth, use an artificial saliva spray to swish and swallow immediately prior to the meal.
- Incorporate Slippery Textures: Add gravies, sauces, or high-quality flavored olive oils to purees and soft foods. This builds moisture and makes items slippery for easier transport down the esophagus. Remember that foods like mashed potatoes become sticky as they cool. Combat this by reheating and mixing in butter, sour cream, and gravy.
- Adhere to Smaller Bite Sizes: Cut meats and vegetables to a maximum size of 1.5 cm for adults (roughly the size of an adult thumbnail) to drastically reduce choking risks.
- Prepare Portable Thickeners: Carry convenient thickener packets, pre-measured containers, and your own measuring spoons to holiday gatherings or summer cookouts. This allows you to discretely adjust liquids, thin broths, or blended soups to your required liquid consistency.
- Adapt the Dining Environment: If you are gathering around a table, reduce chaotic environmental distractions by turning off the television and lowering background music volume. For those with dysphagia who are easily distracted, keep the table setting simple (one plate, one cup, one utensil) to assist those who experience sensory or cognitive overload. Ensure bright lighting and use plates that contrast sharply with the color of the food.
- Maximize Mealtime Success: See this blog by Dr. Samantha Shune, PhD, CCC-SLP that addresses how the shared meal can help engage an at risk older adult, improving socialization, communication, as well as eating and swallowing.
- Minimize Caregiver Burden: See this blog I wrote with Drs. Samantha Shune, PhD, CCC-SLP & Ashwini Namasivayam-MacDonald, PhD, SLP(C), CCC-SLP, Reg. CASLPO on Caring for Caregivers. Make sure to check out the list of resources for caregivers and clinicians at the end of the blog. Don’t miss information on CARES (Caregiver Analysis of Reported Experiences with Swallowing Disorders Screening Tool or CARES) to document and address caregiver burden. See also this article from Shune and team (2025), validating CARES for people with neurodegenerative disease.
See more tips here in my article on Lyons Health Labs and in the Cooking For Dysphagia cookbook noted above.
8. Advocate for Person-Centered Care for All: Real Burden of Dysphagia
Dysphagia that is unaddressed causes poor outcomes, extends people’s lengths of stay in hospitals and skilled nursing facilities, and reduces survival rates (Patel et al., 2018). It also places a significant economic burden on our nation’s healthcare system, elevating costs of care, according to the research by Patel and colleagues (2018). Beyond the financial impact, the emotional toll can cause severe anxiety, depression, and social withdrawal. Food is central to human connection, culture, and celebration.
Dysphagia Awareness Month is more than statistics. It is about more than receiving evaluations and recommendations from your medical team and learning food preparation tips. It is about the person sitting across from you who feels isolated or fearful when eating and swallowing. It is about your loved one who has not had a meal in weeks (or longer). It is about the healthcare providers (SLPs included) providing an appropriate standard of care – or better yet – striving for the best person-centered care, according to the individual in front of them in the clinic.
After reading this Dysphagia Awareness Month’s 5-part series, you are becoming an informed advocate. Here it is again:
- Dysphagia Awareness Month: What You Need to Know
- Rewiring Neurogenic Dysphagia: Finding Hope in the Brain-Swallow Connection
- Deep Dive into Esophageal Dysphagia + 10 Questions
- Hidden Struggle: 7 Updates in Head and Neck Cancer
- This current article: Transform Dysphagia Care: Thrive with 8 Tips on Person-Centered Care.
You have been learning the lingo of dysphagia, the importance of standards like IDDSI, the need for protocols such a nursing swallow screen, and the value of a multidisciplinary team.
When swallowing disorders are left under-identified, under-evaluated, and under-treated, that creates a physical and emotional burden on the person. Treatments that only offer rigid orders and restrictions do not align with person-centered care. The person is at the center of their own medical team, but the burden of advocacy cannot be placed solely on the person with dysphagia.
SLPs must also advocate for thorough care and the informed decision-making process. These communications, trainings, and discussions about the person’s goals of care must be documented. Your rationales for what testing was done or not done must also be documented. Good documentation is good for person-centered care.
What’s Next?
I start the summary with a question. I want to encourage questions. Keep asking: What else?
Now that we have reviewed these foundations of person-centered care, we want to hear from you.
- What is your biggest day-to-day challenge with dysphagia?
- What do you wish your family or healthcare team understood better about your personal journey?
- How have restrictive, one-size-fits-all style recommendations affected you?
- What person-centered care preferences have you shared with your medical team?
Let’s start a supportive conversation in the comments below.
Thank you for reading & sharing!
*******
References:
Garand, K. L. F., McCullough, G., Crary, M., Arvedson, J. C., & Dodrill, P. (2020). Assessment Across the Life Span: The Clinical Swallow Evaluation. American journal of speech-language pathology, 29(2S), 919–933. https://doi.org/10.1044/2020_AJSLP-19-00063
Min, Y., Kim, W. S., Kang, S. S., Choi, J. M., Yeom, J. S., & Paik, N. J. (2016). Incidence of Dysphagia and Serial Videofluoroscopic Swallow Study Findings After Anterior Cervical Discectomy and Fusion: A Prospective Study. Clinical spine surgery, 29(4), E177–E181. https://doi.org/10.1097/BSD.0000000000000060
Molfenter, S. M., Amin, M. R., Balou, M., Herzberg, E. G., & Frempong-Boadu, A. (2023). A scoping review of the methods used to capture dysphagia after anterior cervical discectomy and fusion: the need for a paradigm shift. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 32(3), 969–976. https://doi.org/10.1007/s00586-022-07515-1
Molfenter, S. M., Amin, M. R., Branski, R. C., Brumm, J. D., Hagiwara, M., Roof, S. A., & Lazarus, C. L. (2015). Age-Related Changes in Pharyngeal Lumen Size: A Retrospective MRI Analysis. Dysphagia, 30(3), 321–327. https://doi.org/10.1007/s00455-015-9602-9
Patel, D. A., Krishnaswami, S., Steger, E., Conover, E., Vaezi, M. F., Ciucci, M. R., & Francis, D. O. (2018). Economic and survival burden of dysphagia among inpatients in the United States. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus, 31(1), 1–7. https://doi.org/10.1093/dote/dox131
Shune, S., Gray, L. T., Perry, S., Kosty, D., & Namasivayam-MacDonald, A. (2025). Validation of the Caregiver Analysis of Reported Experiences with Swallowing Disorders (CARES) Screening Tool for Neurodegenerative Disease. American journal of speech-language pathology, 34(2), 633–645. https://doi.org/10.1044/2024_AJSLP-24-00253
Shune, S. E., Resnick, B., Zarit, S. H., & Namasivayam-MacDonald, A. M. (2020). Creation and Initial Validation of the Caregiver Analysis of Reported Experiences with Swallowing Disorders (CARES) Screening Tool. American journal of speech-language pathology, 29(4), 2131–2144. https://doi.org/10.1044/2020_AJSLP-20-00148