
Dysphagia Awareness Month: What You Need to Know
Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction
The month of May was National Speech-Language-Hearing Month (NSLHM), honoring the work of speech-language pathologists across the United States. However, the acronym doesn’t include a “D” for dysphagia: difficulty swallowing. On September 27, 2008, Congress passed a bipartisan statute making June the National Dysphagia Awareness month! So, let’s start this vital conversation.
Swallowing is a complex sequence of anatomy and physiology that most of us perform over 1,000 times a day without a second thought. We swallow to enjoy a meal with friends or family, to sip a morning coffee, and even to clear our own saliva while we sleep. We swallow at least 1.5 liters (1.6 quarts) of saliva a day. But for millions of people, this “automatic” process becomes a daily challenge.
As we step into Dysphagia Awareness Month, SwallowStudy.com will launch our comprehensive weekly blog series. Check out my previous article on dysphagia awareness month here. Over the next four weeks, we will discuss how dysphagia is often misunderstood and frequently overlooked, yet impacts every facet of a person’s life.
This first installment serves as your roadmap. We’ll define what dysphagia is, explore how it happens, and offer a glimpse into the specialized topics we will uncover in the coming weeks. Whether you are a person with dysphagia, a caregiver, or a healthcare professional, this series is designed to empower you with evidence-based knowledge from Karen Sheffler at SwallowStudy.com.
What Exactly is Dysphagia? (The Science of the Swallow)
In the medical world, dysphagia is the formal term for trouble swallowing. It is important to remember that dysphagia is not a disease itself; it is a symptom. Much like a cough can signal a cold or an allergy, dysphagia signals an underlying disruption in the body’s ability to move material safely and efficiently from the mouth to the stomach.
To understand dysphagia, we must understand the three primary “gears” of the swallow. While we will look at these as seemingly separate phases, it is important to know that they work in a synchrony of movement. Even before this motor output of swallowing is triggered, we cannot forget all the sensory input. The first smells and tastes of foods provide important sensory input to start the coordinated motor output. The act of feeding yourself, even if you need assistance, can make your mealtime more successful.
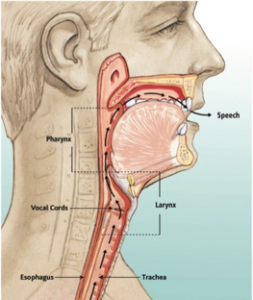
Reprinted by permission of InHealth Technologies (a business of Freudenberg Medical, LLC).
1. The Oral Preparatory & Oral Phases (The “Gateway”)
The Gateway is a good way to think of the first phase of swallowing, as the mouth is the largest hole in the body. It takes in food and liquids, but it can also be a source of bad bacteria that can make you sick. We rely on good saliva and clean teeth, gums, tongue, and palate to make this phase go smoothly. The minute you smell burgers on the grill and even before you take a bite, you build up slippery saliva. That bite requires jaw strength to chomp through its layers and lip strength to keep the food in the mouth. Your tongue and jaw coordination work to chew and form a ball or bolus that is swallow ready. The tongue then has to strip that bolus across the roof of the mouth and back into the throat.
Some signs of dysphagia in this oral phase may be:
- food and liquid falling out of the mouth,
- food or pills pocketing/stuck in the cheeks, or an
- inability or even hesitancy to move the food/liquid/pills to the back of the mouth.
It is important to note that this oral phase is under the person’s control, but you need to be relaxed, have good control, and not be severely short of breath or distracted. Impulsivity, poor attention, and anxiety or fear of swallowing/choking can affect this oral phase. You have to voluntarily control that bolus and push that food, liquid, or pill toward the back of the mouth and into the throat to be able to trigger the pharyngeal swallow response and start the next phase.
Here is a video example of a person who had fear of swallowing pills. You can see her shaking her head “no,” thinking she could not swallow the pill. However, she did not realize that she was actively holding the pill on her tongue. She was fearful to let that pill go into the top of the throat, which was necessary to trigger the swallow.
If you have difficulty with this, see a speech-language pathologist who can use biofeedback to show you your swallow on a live motion video (i.e., videofluoroscopic swallow study or modified barium swallow study).
2. The Pharyngeal Phase (The “Crossroads”)
This is the most critical phase, requiring the most precise timing and coordination. The path of the bolus (green arrows below) meets at a crossroads with the path of breathing (black arrows below).
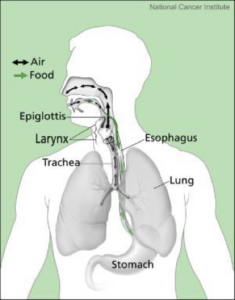
As the bolus enters the throat (pharynx), the brain must coordinate a rapid cascade of events. Here is a simple summary of these complex actions:
- the larynx elevates and moves forward (feel your Adam’s apple move up in your neck when you swallow);
- the vocal cords close off to protect the airway;
- the soft palate rises to block off the nasal passage (you don’t want liquid up in your nose);
- the tongue base pushes into the back wall of the throat (pharynx), starting a squeezing wave or peristaltic action to efficiently strip the bolus through the throat. Your ability to clear the bolus through the throat is called the swallow efficiency.
- this pushing action of the tongue and squeezing action of the throat, in addition to the upward and forward movement of the larynx all help to close up the top of the airway (laryngeal vestibule). Your ability to seal up the top of the airway is called the swallow safety.
- The epiglottis flips down as a response to the movement, squeezing actions, and pressures from the bolus. It is a mechanical lever and not a muscle.
- Don’t let Google, AI, or your doctor blame just the epiglottis if you have reduced airway protection.
- You may need to work with your speech-language pathologist on your timing, coordination, strength, and pressures from different sizes and textures of the bolus. There is no exercise just for the epiglottis!
Signs of dysphagia in this pharyngeal phase may be:
- Penetration: Food or liquid entering the top of the laryngeal vestibule (when the item is still above the vocal cords);
- Aspiration: Food or liquid falling below the vocal cords into the trachea to lungs (which can happen silently, without you feeling the urge to cough or clear your throat). This is referred to as a safety problem.
- Residue: If the peristaltic squeezing action is reduced, you may have food, liquid, pills, or saliva left behind in pockets in your throat or along the walls of the throat. This is referred to as an efficiency problem.
3. The Esophageal Phase (The “Final Stretch”)
Once the bolus passes the throat, it enters the esophagus (the food tube) via the upper esophageal sphincter. The elevation action of the larynx yanks open the sphincter (also known as the pharyngoesophageal segment) after it gets the message from the brainstem to relax. Then, the pushing actions and pressures of the bolus help to distend/stretch open this sphincter.
The esophagus is the final stretch on the journey to the stomach. Through waves of muscular contraction (peristalsis), the food is squeezed down into the stomach.
Many people experience a sensation of food getting “stuck” in their chest or a feeling of “slow transit.” Very often, a person feels food sticking high up in their neck and even has fear of choking, when the food is actually stuck much lower down in the esophagus. This is called a referred sensation, as the esophagus is not very smart when it comes to detecting sensation. You may have food stuck low in your esophagus (like in a hiatal hernia or at an esophageal stricture/narrowing), but you may feel it up in your neck. Sometimes this is felt around the larynx (adam’s apple) or just below in that indentation called the sternal notch.
This lingering lump-in-the-throat sensation is called a globus sensation. Frequently, it is felt when someone has severe reflux or silent reflux that gets up high in the throat – especially at night. Please see the Reflux Severity Index (RSI by Belafsky, et al, 2002) that goes over some of these symptoms of gastroesophageal reflux disease (GERD) and laryngopharyngeal reflux (LPR).
While esophageal issues are managed by gastroenterologists, the Medical Speech-Language Pathologist (SLP) plays a vital role in identifying when the dysphagia is up in the oral and pharyngeal phases or if it is an esophageal issue OR BOTH. Sometimes the pharynx impacts the esophagus. Or, the esophagus can cause problems in the pharynx (especially if that food or liquid is shooting back up into the bottom of your throat). The SLP uses the modified barium swallow for a multi-phase comprehensive dysphagia evaluation with scanning the esophagus (after liquid, food, pills) to see if the person’s sensations match the findings on x-ray.
Please see my prior blog on making sure the SLP scans the esophagus during the videoflouroscopic swallow study (aka, modified barium swallow study), to make appropriate recommendations and referrals.
Again, that x-ray can speak 1000 words, as people can watch that that motion video live during the modified barium swallow study (biofeedback). It is important to learn where the food is actually getting stuck, and reconnect that with the sensations you are having. That is an important step in reducing hypersensitivities and fear of swallowing. Watching your swallowing can really relieve your fears of choking if the food is actually getting stuck lower in the esophagus. The goal for many in this situation is to slowly reduce the anxiety and enjoy eating again by using simple strategies like a slower rate and alternating with liquids, for examples. Your SLP and the rest of your medical team will work with you on your individual issues and goals.
Why Dysphagia Awareness Matters: The High Stakes of Swallowing Disorders
If someone has trouble walking, they might use a cane. If they have trouble seeing, they get glasses. But if someone has trouble swallowing, the consequences can go undetected and be life-threatening. Often, people do not know that they have difficulty swallowing, as sensation of residue can be poor and liquids can get down the wrong way silently (silent aspiration). See “How do I know that I or my loved one may need a swallowing evaluation?”
Additionally, if someone falls, the doctor automatically orders an x-ray to detect if anything is broken and what to do about it. If someone has a fever, cough, and sputum production, the doctor orders a chest x-ray to detect pneumonia. However, when someone has difficulty swallowing, they often do not get a referral to a speech-language pathologist who specializes in swallowing to receive comprehensive testing. The SLP needs a doctor’s order for any testing. The testing may include what we call “instrumental assessment,” using motion x-ray or a flexible endoscope. SLPs like to remind people that we do not have x-ray vision and cannot determine the type or severity of the dysphagia and aspiration just by watching someone eat/drink. I have been working in dysphagia for 30 years, and I still do not have x-ray vision! The bedside swallowing evaluation may be the place to start, but the SLP then needs to determine if the instrumental assessment is needed and warranted (i.e., modified barium swallow and fiberoptic endoscopic evaluation of swallowing). Sometimes, further testing is not warranted clinically. The SLP and medical team will take into considerations your wishes for further testing or not. Regardless, the SLP should provide and document the rationale for why further testing or why not. The SLP also provides important education and communication with the medical team, making necessary referrals to other disciplines that work on all aspects of feeding, eating, and swallowing.
Let’s review some of the potential outcomes of dysphagia:
- Aspiration Pneumonia: When food, liquid, or saliva, along with that nasty oral bacteria enter the lungs, it can lead to a serious lung infection, especially if the person has decreased immune responses. This is one of the leading causes of hospitalization for elderly patients and those with neurological conditions. Reflux or regurgitation can also come back up during meals, after meals, and when lying down and cause pneumonia or pneumonitis. It is important to state that aspiration does not automatically equal pneumonia. Please consider these 3-pillars of aspiration pneumonia by Dr. John Ashford. See this blog on oral health.
- Malnutrition and Dehydration: If eating is painful or difficult, people naturally eat and drink less. This can lead to a downward spiral of muscle wasting (sarcopenia), which then can make swallowing even harder from deconditioning. Not drinking enough fluids can cause dry mouth, exacerbating any dry mouth issues you may have from medication side effects. When dehydration continues, it can cause headaches, cognitive problems, brain fog, dizziness, muscle cramps. Then, if left untreated, dehydration can cause serious issues like: kidney failure, seizures, shock from not enough fluid in the blood, and worse.
- Social Isolation and impact on your quality of life: So much of our human connection happens over food — birthdays, weddings, holidays. When you can’t eat what everyone else is eating, that places a burden on you and your loved ones. Please see this blog regarding caregiver burden and resources.
- Choking Risks: Actual choking is a complete airway blockage from food or an object that prevents any air passage or breathing. This is called asphyxiation. The person will not be able to breathe or cough, and they may be giving the universal sign of choking of hands encircling their neck. See this image below of a piece of bread stuck at the top of the airway in the voice box / larynx (aka, laryngeal vestibule above the vocal cords).

Image excerpt from IDDSI’s full YouTube video: https://youtu.be/W7bOufqmz18
-
- Choking is a terrifying emergency, requiring very rapid action to relieve the obstruction. If you are a caregiver for someone who is at risk for choking on their food, it is important to be trained in CPR and Basic First Aid, which must include choking relief protocols for infants, children and adults, as each group has specific guidelines. Please see my prior article on choking and the risks with bread.
When choking or airway blockage (asphyxiation) unfortunately leads to poor outcomes or even death, that may or may not have been due to actual negligence or wrong-doing. Explaining these complexities of dysphagia and understanding the standard of care for reducing risks for choking and aspiration pneumonia is a cornerstone of what we do as dysphagia expert witnesses. Note: aspiration and choking cannot be prevented 100% of the time.
Special Segment ~ When that choking sensation is not actual airway blockage:
It is important to differentiate actual airway blockage from when people say: “I choked on my water,” as that is likely just drops of water poking into the top of the airway causing you to cough and try to eject that penetration or aspiration. That is not actual airway blockage. In this scenario, the cough is a good thing. Encourage the cough, as this is the body’s airway protection strategy.
Frequently, people feel like they are at risk for choking due to a “globus sensation,” or feeling a lump in the throat. This may come on in response to chronic and prolonged coughing that can sometimes become a habit. It may start from refluxing events. As noted above in the esophageal section, sometimes people get the sense that they are “choking on food” when the food is actually stuck farther down in the esophagus.
You may fear “choking,” when the risk is not actually present. The body can play tricks on you and get you into maladaptive patterns. Chronic cough can become a vicious cycle, as the more you cough, the more swollen the tissues become, and the more you feel something “stuck.” Chronic coughing and muscle tension can result in a laryngeal spasm, where the vocal cords tense or close up. This may last for up to 1 minute or so, but it can be relieved with pursed-lip breathing (in through the nose and out the mouth through pursed lips or sniffing that can relax the vocal cords into a wide open position).
If this happens to you, please see an Ear, Nose, and Throat doctor (ENT) and a speech pathologist. The SLP should specialize in voice, reducing muscle tension, and quieting the chronic cough.
Preview: Our Weekly Deep-Dive Series
Dysphagia doesn’t discriminate. It affects everyone from premature infants to the elderly. However, the causes of dysphagia define the treatment. Performing a good comprehensive dysphagia evaluation is the first step in treatment, as the medical team needs to figure out what are the underlying causes of this symptom known as dysphagia. Then, the foundation of dysphagia treatment/management is a person-centered care approach. You are at the center of your medical team. You should review findings with your medical team and seek answers to all your questions before making informed decisions about your care.
Over the next month, we will introduce you to some of these underlying causes of dysphagia. We noted above that dysphagia is a symptom of other issues, disorders, diseases, or anatomical abnormalities. Building your understanding of the underlying issues will help you advocate for yourself as part of your medical team!
Week 1: Neurogenic (Neurological) Dysphagia
The brain is the “conductor” of the swallowing orchestra. When there is a “short circuit” due to a Stroke, Parkinson’s Disease, ALS (Lou Gehrig’s Disease), or Multiple Sclerosis, the muscles of the face, mouth and throat may be weak or they may not be getting the right signals at the right time.
Week 2: Gastrointestinal (GI): Esophageal Structural & Motility Issues
Sometimes the problem isn’t at the top of the throat; it’s further down. We will explore how chronic reflux (GERD), laryngopharyngeal reflux (LPR), esophageal strictures, Eosinophilic Esophagitis (EoE), and motility disorders can cause that “stuck” feeling and “globus sensation.” Have you ever felt like a piece of steak was stuck behind your breastbone? Do you feel a backflow or regurgitation after meals? Do you wake up coughing in the middle of the night, have a bitter taste in the mouth in the morning, and clear your throat all day long? We already touched on some of these issues above in this blog.
Week 3: Cancer & Survivorship (Head and Neck Oncology)
Treating cancer—while life-saving—can be incredibly hard on the swallowing mechanism. Surgery can remove vital structures, and radiation can lead to Radiation-Associated Dysphagia (RAD), which causes scarring and stiffness (fibrosis). We will discuss how to manage swallowing before, during, and after cancer treatment to ensure the best long-term quality of life.
Week 4: How to Live (and Thrive) with Dysphagia
If you or a loved one has recently been diagnosed with a swallowing disorder, the first thing you need to know is: You are not alone, and this is not the end of your relationship with food. Living with dysphagia is about advocating for comprehensive evaluations, learning and adaptation as needed, and potentially rehabilitation. It is not just about restriction.