
Bread of Life? Evidence on Choking Risks with Bread
by Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
in collaboration with Dr. Catriona M. Steele, PhD, CCC-SLP, ASHA Fellow,
Dr. Julie Cichero, BA, BSpThy (Hons), PhD, and
Laura Brooks, MS, CCC-SLP, BCS-S (on behalf of the Communications and Advocacy Work Group of the USIRG)
Introduction to the Choking Risks with Bread
We often hear bread referred to as “the bread of life.” A quick google search shows at least 25 quotes on the “bread of life” from Mother Teresa to Mahatma Gandhi. Gandhi has been quoted as saying: “There are people in the world so hungry, that God cannot appear to them except in the form of bread.” Bread has achieved quite an elevated status. However, in the world of swallowing disorders (dysphagia), bread is known as one of the most chokable foods. Therefore, it is so important to analyze it from an eating and swallowing safety standpoint, especially as bread can not only give life, but it can take a life too — in the form of a choking event (airway blockage or asphyxiation)! This article will address the choking risks with bread and its many complexities.
So, fortunately, the Scottish writer, D.W. Brogan, said: A person “does not live by bread alone, even pre-sliced bread.”

This blog was inspired by a recent question on American Speech-Language & Hearing Association’s (ASHA) SIG 13 online community page from a speech-language pathologist (SLP), Gavin Levy, asking: Why does bread so often appear on texture-modified diets (dysphagia diets) in healthcare facilities? He noted that it should only be on a Regular level diet. Is there such a thing as “soft bread,” and is toast any easier or harder to process in the mouth (oral processing) and swallow through the throat (pharyngeal swallowing) than other breads? Many SLPs are making that distinction, but is “soft” bread safer and acceptable for someone on an altered diet?
The easy answer:
Based on a decade of work, which is backed by 50 years of research, the International Dysphagia Diet Standardisation Initiative (IDDSI) has stated that all bread is a Regular, Level 7 food item.
In Depth Review of Choking Risks with Bread
Bread is a hot topic, and these questions led to great discussions among members of our United States IDDSI Reference Group (USIRG) and two of the IDDSI global board members and dysphagia experts: Dr. Catriona Steele and Dr. Julie Cichero. We addressed the oral processing and pharyngeal phase issues with bread and the inherent choking risks with bread. I will try my best to share facts, references, and expert opinions from these esteemed speech pathologists and IDDSI.
What Does IDDSI Say on the Choking Risks with Bread?
First, let’s start by referring to the IDDSI Framework (found on www.IDDSI.org in the IDDSI Standards tab), which describes bread as a Regular, IDDSI Level 7 food item in the Complete IDDSI Detailed Definitions document. (Full English Link: https://cms.iddsi.org/media/publications-iddsi/detaileddesriptions/english/V2DetailedDefnEnglish31july2019.pdf)
IDDSI’s Frequently Asked Questions tab (filter by “Foods”) highlights research and coroner’s report findings that breads and meats pose the biggest choking risk. Here is text directly from the IDDSI.org website:
“As a general rule bread products are considered a regular food texture (Level 7). This decision is based on the choking literature where bread is often identified as a cause of choking (Irwin et al., 1977; Ekberg & Feinberg, 1992; South Australia Coronial Inquest, 1997; Wick et al., 2006; Berzlanovich et al., 1999, 2005; Food Safety Commission of Japan, 2010; Licea, 2016). Bread and sandwiches require the ability to both bite and chew. Although bread looks and feels soft, it cannot be easily mashed or broken down into particles of 4mm or smaller due to its fibrous nature. In fact, the number of chewing strokes, chewing strength and stamina required to make bread swallow-safe are about the same as those required to chew and swallow peanuts safely (Hoebler et al., 2000; Koyama et al., 2003). Individuals who tire easily while chewing may find bread difficult to chew to a small enough size to be swallow-safe. Bread also requires softening with saliva for effective chewing (Hoebler et al., 2000). For individuals with dry mouth (e.g., medication side effects, post radiotherapy, etc.) bread is often not adequately wetted for swallowing resulting in food sticking in the throat. Bread does not dissolve when wet but does become sticky. Sticky or adhesive foods are also considered a choking risk (Irwin et al., 1977; Ekberg & Feinberg, 1992; Wick et al., 2006; Berzlanovich et al., 1999, 2005). The ability to safely manage bread and sandwiches should be assessed on a case-by-case basis by a dysphagia specialist.” (References at the end of this article.)
Let’s Hear More from the Experts:
Slimy & Sticky – Not Soft
Dr. Steele described this issue of stickiness further in our discussion: “The reality is that bread comes in all sorts of textures around the world and may behave differently based on flour, fat content, etc. If one is talking about regular sandwich bread in North America (e.g., typical white sandwich bread), the product tends to quickly become slimy and gummy in the mouth, and it does not actually break down very easily.”
Dr. Cichero agreed and had a lot to share with us about the complexity of bread and its choking risks: “Bread is considered by many people to be ‘soft’. Even ‘soft’ looking and feeling bread has fibers that you cannot mash with a fork (see the IDDSI Fork Pressure Test on YouTube, showing the pressure testing can be done with chopsticks and finger/thumb too).”
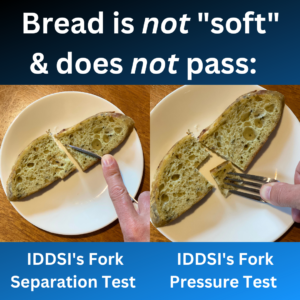
See IDDSI’s Testing Methods here (such as the Fork Separation Test and the Fork Pressure Test): https://iddsi.org/Testing-Methods
Dr. Cichero continued: “You need a knife to cut bread, or you use your fingers to rip or break bread. The initial bite down into some bread gives the impression that it is a soft texture. Bread that has been prepared with high aeration is the type of bread that when cut has holes in the loaf. Then there is dense bread like rye, that is not soft at all. We are using the term ‘bread’ as a catch-all to discuss potentially very different textures.”
Dr. Cichero added: “What tends to happen is that saliva coats the bread bolus, and this gives it a slippery texture. The oral sensory receptors identify that it is slippery, and this is one of the triggers that a bolus is ‘prepared and ready to be swallowed’.”
Is this the reason why people tend to swallow bread before it is swallow ready?
“Yes,” answered Cichero, “and while the outside is slippery, the inside of the bolus is dry and firm. Sure, the outside may feel slippery, but because of the gluten in bread it is also sticky. It will not break down into particles (particulate) when swallowed, so it will remain as a ball or glob (called a bolus). If the bolus is large, it may obstruct the airway, causing a choking event.”
“At this point we are just talking about the bread, let alone any filling that might be placed in the middle of two pieces of bread. This represents a complex and challenging mixed texture that is firm, slippery and sticky.”
Of course, we must also ask: What if the person has very low saliva quantity and altered saliva quality (chemistry)? That really elevates the risks!
Bite Force and Oral Processing
“Bread requires about 30 chewing strokes to break the particle size down and to mix it with saliva. This about the same number of chewing strokes as a piece of apple,” per Dr. Cichero.
“You need sufficient bite force to ‘cut bread’ with your teeth and molar function to masticate and break the fibers and particles. With fewer than 13 teeth there is an increased choking risk on all substances, but especially bread and meat according to coroner’s reports and research findings. For people who have dentures, they have a reduced ability to break food particles down and tend to swallow food pieces that are large. Therefore, in some people with altered dentition, there may be an increased choking risk for the reasons noted above.”
In her article in 2018, Cichero addresses these dentition issues alongside the complex and multifactorial issues that go into choking risks. She noted in the article how “sobering” it is “that after falls (being the first highest cause), choking on food presents as the second highest cause of preventable death in aged care (Ibrahim et al., 2015).” I highly recommend this 2018 review paper, which addressed not only the choking risks in the frail elderly, but also the need to balance the discussion of risks with person-centered care and the person’s autonomy in their shared decision-making about their own healthcare. More on person-centered care towards the end of this article.
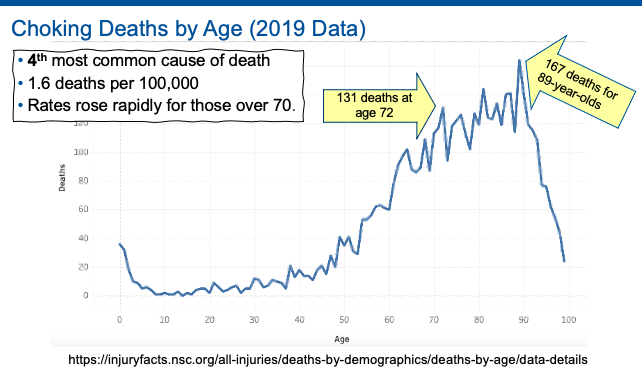
Choking on food is the 2nd highest cause of preventable death in aged care (Ibrahim et al., 2015), only second to falls. Choking is the 4th most common cause of death.
What About Toast?
“When we heat bread, the heat softens it. When we add a fat like butter or margarine, this interacts with the gluten and makes the fibers softer. However, if heated bread (toast) becomes cold, it becomes hard. Bread is a very complex texture,” summarized Dr. Cichero.
Comfort Food, Nutrition & Bread Alternatives
Dr. Cichero made some great points here: “Bread is a staple of many western diets and as such it is a ‘comfort food’ and is good for mealtime compliance. It is favored by our dietetic colleagues for the calories that it provides, as well as the fact that bread is often enriched with important vitamins and minerals. IDDSI went to special efforts to see how we could change the texture of bread and sandwiches to ensure they could be swallowed safer. This is where the IDDSI Minced & Moist, Level 5 recipe and YouTube video came from.”
Image excerpt from IDDSI’s full YouTube video: https://youtu.be/W7bOufqmz18.
Makes a great short training video on the choking risks with bread and the solution for a bread alternative.
Based on Drs. Steele and Cichero’s work, as well as the IDDSI framework that is backed by years of research, IDDSI strongly advocates for the use of this Minced & Moist Bread Recipe for people who want bread and are on Minced & Moist, Level 5 or Soft & Bite Sized, Level 6.
Careful with Snack Time!
Drs. Steele and Cichero both urged healthcare staff to remember that this choking risk is not only present at typical mealtimes, but at snack times as well. Many facilities and residential care homes have bread accessible for snacks in their on-unit kitchens, noted Dr. Steele. “This is an important point to share as it may be a time when there are fewer people around to supervise and/or intervene if a choking event occurs. Also, it can be potentially problematic whenever the normal routine is disrupted, such as during special occasions and facility events,” reminded Dr. Cichero.
How Do SLPs Evaluate Choking Risks with Bread?
“The clinical swallowing assessment cannot solely focus on liquid swallowing and signs of aspiration,” stated Dr. Steele. “The clinician must have a standard of practice with respect to evaluating chewing, oral processing, and swallowing of foods.”
“We can and should do better,” said Dr. Steele.
“I agree that we have focused so heavily on liquids,” added Dr. Cichero. “It is now time to make sure our skills with evaluating oral processing function and safety for solids should be honed and come to the fore.”
Bedside Evaluation for Oral Processing Skills
Per Dr. Steele: “I would say that the most objective current approach for determining whether a patient has the necessary oral processing skills to handle a particular bread (or, for that matter, any type of solid), is to evaluate them at the bedside/tableside while consuming a whole sandwich or bread item.
Ask them to chew the food until the point where they think they are ready to swallow, and then either ask them to open their mouths so you can inspect the food, or have them spit it out, and do IDDSI testing on the expectorated bolus. These suggestions are made in two recent articles (Bandini et al., 2022; Cichero, 2020).”
See also this prior article on SwallowStudy.com called: “Diet Modification Without Mastication Evaluation?”
Dr. Cichero adds: “My strong recommendation for SLPs who wish to provide bread is that they sit with the person and evaluate the following:
- Ability to bite down and bite off a piece of food that is of suitable size,
- Chewing strength, and
- Stamina through a meal.
- Inspect the bolus once the person thinks it is ready to be swallowed.
- Evaluate chewing and oral processing skills during the meal/entire sandwich if that is what the person will be served as recommended by the SLP.
- Does the person chew sufficiently?
- Do they eat very fast?
- Do they put too much food in their mouth?”
“Impulsivity, shoveling, and other potentially dangerous behaviors — when combined with complex textures like bread — can increase the risk of choking.”
SLPs have known the above for decades; that is our standard of care to assess for those points. This is now a matter of highlighting risks, unifying practice patterns, and honing skills.
Instrumental Evaluation of Bread
One could also use a Flexible Endoscopic Evaluation of Swallowing (FEES) to give further information about the pharyngeal skills when swallowing bread. Dr. Steele advised that the use of FEES to assess bread is “probably a better assessment for looking at the state of the bolus after oral processing and for looking at pharyngeal phase function on bread.”
This FEES video shows the dangers of fast eating with minimal oral processing when eating bread.
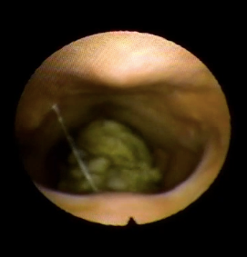
Above video and this image are shared with permission from Katrina Woodward, MS, CCC-SLP, CDP, of SDX Dysphagia Experts and VP of Education and Planning for the Massachusetts Speech-Language-Hearing Association.
In this video and still image from the FEES (Flexible/Fiberoptic Endoscopic Evaluation of Swallowing), you see an endoscopic image of the swallowing structures: the base of the tongue that forms the front part of the pharynx, the back and side walls of the pharynx, and the larynx or laryngeal vestibule that ends at the vocal cords, which are the gateway into the trachea and lungs below. This study shows the back wall of the throat/pharynx at the top of the image and the tongue base, epiglottis, and the front of the throat at the bottom of the image. This person was eating a slice of bread quickly and impulsively without adequate chewing. You see globs of partially chewed bread falling into the pharynx towards the top of the airway (into the laryngeal vestibule). Since the bread appeared to be in this vestibule but still above the level of the vocal cords, the person could still cough forcefully to eject it. However, forceful ejection requires good alertness, safety awareness, good sensation of this airway invasion, and a very good respiratory effort cough and expectorate.
Note: This current blog addresses the oral processing and pharyngeal phase issues and evaluations with bread. It does not even address the esophageal aspects of clearance through the food tube (esophagus) to the stomach, but we do know that bread and meat are common items that can be retained in the esophagus if there is a structural abnormality, like a narrowing, or an esophageal dysmotility. The videofluoroscopic swallow study assesses solids in the oral phase through the pharyngoesophageal phases. The esophagus can be scanned and rated using the MBSImP (Martin-Harris et al., 2008) ratings of esophageal retention and if there is backflow (aka, retrograde flow) and up to what level. With that backflow risk, does the food and/or liquid come back up to the upper esophagus or all the way to the lower pharynx, which could cause serious choking risks? This consideration needs to be a part of your comprehensive evaluations. Please see also other blogs on esophageal dysphagia and multiphase pharyngoesophageal testing with the REST protocol. It is important to refer appropriately to a gastroenterologist with any suspected esophageal concerns.
Dr. Catriona Steele reminds us: “The IDDSI Framework is intended to describe food and liquid characteristics and it is not intended to be prescriptive in terms of recommending particular food items for inclusion either in diets or for use in assessment. Esophageal function and the utility of specific foods for evaluating esophageal motility were not considered during the development of the IDDSI Framework.”
Evaluations Need to Determine Level of Supervision
Dr. Cichero reinforced the need to address the level of supervision in the recommendations after a swallowing evaluation. “The SLP should also determine whether supervision is required. They should discuss risk mitigation strategies and plan with nursing staff, care staff, caregivers, and family members (healthcare proxies) how they will handle a choking event if it were to occur.”
Not the Sandwich Police:
Ultimately, IDDSI and the SLP do not “police” people when they are eating and drinking, telling them what they are allowed to have and not allowed to have. Yes, living in Massachusetts, we know about a town called “Sandwich” on Cape Cod!
Instead, the SLP uses evidence-based practice, which includes a wide breadth of information and research, clinical expertise, and the person’s goals of care/values/preferences.
The speech-language pathologist specializing in dysphagia (SLP) does the following:
- Performs evaluations, which are as comprehensive as needed, indicated and desired;
- Makes recommendations for safer options. Often, there is no “safest” or perfect option. However, these options are provided within a range of curative through palliative approaches. An aggressive or curative approach will be where the medical team is trying to reduce or mitigate risks, potentially at all costs. Keep in mind that person is part of and at the center of this team. The range of options offered goes through more palliative or comfort care approaches based on the person’s goals of care;
- Encourages thorough conversations about these complex risk/benefit decisions; and
- Directs the person (and/or healthcare proxy) to their medical team for the final discussions, informed decision-making, and documentation.
Therefore, the comprehensive dysphagia evaluations may reveal that bread and other regular solid foods will pose a significant risk for residue and choking; however, the person (and/or healthcare proxy) may make an informed decision to continue with regular foods as tolerated to preserve their quality of life and honor their right to choose (autonomy).
Dr. Cichero advised: “All of this information should be documented. We can and should provide person-centered care; however, there should be thorough conversations and documentation for informed consent and consideration of the risks.”
Please see the person-centered care statement created by USIRG (2023):
PERSON-CENTERED CARE (PCC) STATEMENT
The IDDSI Framework cannot change, but the diet order can be individualized. Person-centered diet orders specify an individual’s needs within and outside the IDDSI Framework. The medical team works in collaboration with the person’s wishes, preferences, goals of care, and individual abilities. Risks and benefits may be addressed in the informed consent process. Clear orders, communication, and documentation are key to person-centered care.
Please see this webinar created by Karen Sheffler and Yvette McCoy on MedbridgeEducation called: “Reframing Dysphagia Documentation with a Person-Centered Care Approach” https://www.medbridge.com/course-catalog/details/reframing-dysphagia-documentation-with-a-person-centered-approach-karen-sheffler-yvette-mccoy/ (Disclosure: we do make a small commission on the purchase of the webinar to compensate for the hours that went into the design of the webinar and all the resources that are included). You can watch the first chapter for free!
Summary & Bottom Line on the Choking Risks with Bread:
SLPs have been trained that bread has inherent choking risks due to difficulty with oral processing and pharyngeal swallowing. However, this SLP in the ASHA Listserve, Gavin Levy, highlighted how sometimes our best-practice standards do not always translate into a “unified consensus” in practice patterns in all SLPs across the country or around the world.
The overarching goal of IDDSI for a decade has been: A global consensus on a standardised framework of diet level labels, definitions of food and liquid textures, and testing methods to promote safety for people with dysphagia. IDDSI formed in 2013 and the framework was first published in 2016. This is not new information. IDDSI has had the full support since 2017 of the American Speech-Language Hearing Association (ASHA), the Academy of Nutrition & Dietetics (AND, and Association of Nutrition & Foodservice Professionals (ANFP), who all urged implementation in the United States to start May 2019. As of October 2021, IDDSI became the only professionally-nationally recognized diet framework, per the AND. Of course the COVID-19 pandemic slowed down implementation efforts in many facilities, but these organizations reiterated support in 2022. Adoption in other countries has been ahead of the United States.
Consider how in 2019, two states in Australia already mandated that bread cannot be included on “soft” diets due to choking deaths there. Proactive guidelines are always better at saving more lives than retroactively changing policies after someone dies from a choking event.
*******
Learn More:
- Terrific article: Dr. Julie Cichero, who – again – is a speech pathologist from Australia, and Peter Lam, RD, CFE (the original co-chairs of IDDSI) recommended an article they wrote in 2018: What’s the evidence? Can bread ever be compatible with a texture modified diet?
- FAQs:
- See IDDSI global’s FAQs here: https://iddsi.org/FAQ/Foods – you will find the FAQ regarding bread and other information on foods. Use the left-hand side-bar for other FAQ topics.
- Please see the other FAQs in our USIRG chart of resources, including one on Gelatin/Jell-O that inspired the person-centered care statement by USIRG above: https://iddsi.org/around-the-world/united-states.
- Please see the (USIRG) FAQ on Bread & Mixed Consistencies that is meant to be an adjunct to the resources already on the IDDSI.org website: https://cms.iddsi.org/media/aroundtheworld/usa/usirgfaqexceptionsbreadsmixedconsistencynov2024.pdf
- USIRG Handout with a focus on mixed consistencies and bread: https://cms.iddsi.org/media/aroundtheworld/usa/iddsi-s-focus-on-safety-with-mixed-consistency-foods-bread.pdf
- References gathered by IDDSI & USIRG on Risks of Choking: https://cms.iddsi.org/media/aroundtheworld/usa/resources-for-associated-risks-of-choking-in-adults-and-children.pdf
- Let us know what resources would be helpful for your US specific IDDSI needs. If you have best practices questions, email us at “usa.bestpractices at IDDSI dot net.” This email is also listed at the bottom of our USIRG resources chart: https://iddsi.org/around-the-world/united-states.
References on Choking Risks with Bread & Other Items:
Minced & Moist Sandwich: https://youtu.be/W7bOufqmz18
Bandini, A., Gandhi, P., Sutton, D., & Steele, C. M. (2022). Bolus Texture Testing as a Clinical Method for Evaluating Food Oral Processing and Choking Risk: A Pilot Study. American journal of speech-language pathology, 31(6), 2806–2816. https://doi.org/10.1044/2022_AJSLP-22-00014
Berzlanovich, A.M., Muhm, M., Sim, E. & Bauer, G. (1999). Foreign body asphyxiation – an autopsy study. American Journal of Medicine, 107, 351-355.
Berzlanovich, A.M., Fazeny-Dorner, B., Waldhoer, T. & Fasching, P. (2005). Foreign body asphyxia: A preventable cause of death in the elderly. American Journal of Preventive Medicine, 28, 65-69.
Cichero J. A. Y. (2018). Age-Related Changes to Eating and Swallowing Impact Frailty: Aspiration, Choking Risk, Modified Food Texture and Autonomy of Choice. Geriatrics (Basel, Switzerland), 3(4), 69. https://doi.org/10.3390/geriatrics3040069
Cichero, J. A. Y. (2020). Evaluating chewing function: Expanding the dysphagia field using food oral processing and the IDDSI framework. Journal of texture studies, 51(1), 56–66. https://doi.org/10.1111/jtxs.12462
Ekberg, O. & Feinberg, M. (1992). Clinical and demographic data in 75 patients with near-fatal choking episodes. Dysphagia, 7, 205-208.
Food Safety Commission, Japan. Risk Assessment Report: Choking accidents caused by foods. 2010. https://www.fsc.go.jp/english/topics/choking_accidents_caused_by_foods.pdf (accessed April 2014).
Hoebler, C., Devaux, M.F., Karinthi, A., Belleville, C. & Barry, J.L. (2000). Particle size of solid food after human mastication and in vitro simultation of oral breakdown. International Journal of Food Sciences and Nutrition, 51, 353-366.
Ibrahim, J. E., Murphy, B. J., Bugeja, L., & Ranson, D. (2015). Nature and extent of external-cause deaths of nursing home residents in Victoria, Australia. Journal of the American Geriatrics Society, 63(5), 954–962. https://doi.org/10.1111/jgs.13377
Irwin, R.S., Ashba, J.K., Braman, S.S., Lee, H.Y. & Corrao, W.M. (1977). Food asphyxiation in hospitalized patients. JAMA, 237, 2744-2745.
Kohyama, K., Mioche, L., Bourdiol, P. (2003). Influence of age and dental status on chewing behaviour studied by EMG recordings during consumption of various food samples. Gerodontology, 20(1), 15-23.
Licea, M. & Klein, M. (2016). Patient chokes to death after hospital feeds her sandwich she can’t eat: New York Post: News Corp. http://nypost.com/2016/06/19/patient-chokes-to-death-after-hospital-feeds-her-sandwich-she-cant-eat/ Access date: June 21, 2016.
Martin-Harris, B., Brodsky, M. B., Michel, Y., Castell, D. O., Schleicher, M., Sandidge, J., Maxwell, R., & Blair, J. (2008). MBS measurement tool for swallow impairment–MBSImp: establishing a standard. Dysphagia, 23(4), 392–405. https://doi.org/10.1007/s00455-008-9185-9
South Australia: Coronial Inquest, Dimitra Damianou. 1997 http://www.courts.sa.gov.au/CoronersFindings/Lists/Coroners%20Findings/Attachments/284/DAMIANOU%20Dimitra.pdf Access date: June 21, 2016.
Wick, R., Gilbert, J.D. & Byard, R.W. (2006). Café coronary syndrome-fatal choking on food: An autopsy approach. Journal of Clinical Forensic Medicine, 13, 135-138.