
IDDSI: Interview with an Early Adopter
by Karen M. Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction
I had the pleasure to speak with Kim Bradley, PhD, SLP reg.CASLPO, who is a speech-language pathologist (SLP) and manager at St. Michael’s Hospital in Toronto, Canada. Bradley is also an Assistant Professor in the Department of Speech Language Pathology at the University of Toronto. I asked her: Why was it so important for you and your healthcare facility be early implementors of this new IDDSI framework? Here is what she said:
“As SLPs, we are always looking for the best way to care for our patients. For the patient with dysphagia who has had enough risk with impaired swallowing, compromised nutrition and exposure to X-ray, we felt like we could be doing better – by changing the things we can change and are within our control. Standardizing the terminology contributes to enhanced patient care and safety.”

GLOBAL EFFORT TO IMPROVE PATIENT SAFETY FOR PEOPLE WITH DIFFICULTY SWALLOWING (DYSPHAGIA).
Dr Catriona Steele, PhD, CCC-SLP, BCS-S, S-LP(C), reg.CASLPO, ASHA Fellow, and member of the IDDSI board of directors urged the world healthcare community to “become part of this wave of implementing global terminology for dysphagia diets” (during her ASHA IDDSI lecture in February 2017).
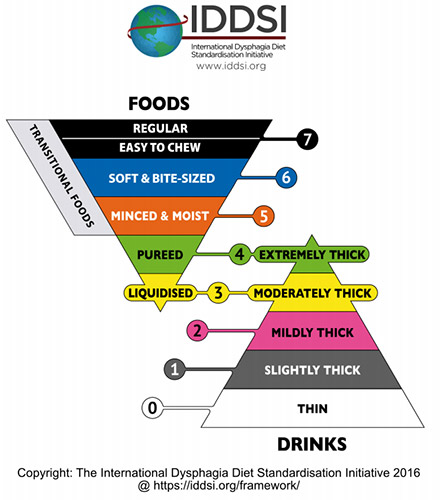
Let’s Learn More About the IDDSI Framework First
To get up-to-date with the International Dysphagia Diet Standardisation Initiative (IDDSI), here are a few helpful links:
- Resource page on IDDSI. Print posters about the IDDSI Flow Test, the Framework, descriptors and testing methods and more. Read IDDSI’s publications. Check out their E-bites Newsletters.
- Prior SwallowStudy.com blogs:
- Diet Safety: Terminology & Definitions Matter (January, 2015)
- “No Dysphagia Diet Modification Without Standardization!” (September, 2015)
- Recipes for People with Dysphagia (with a special analysis of recipes according to the IDDSI Framework) (June, 2017)
- Look into the future with these newer blogs on SwallowStudy.com:
- Diet Modification Without Mastication Evaluation?
- Cotton Candy Therapy? Transitional Foods & Dysphagia Treatment
- Patient Safety First: Transitional Foods (Part 2)
- Jelly & Jell-O Surprise: What’s Up With Jell-O, Jelly Cups, Dysphagia Training Jelly (Part 3 of Transitional Foods Series)
- The master guidance blog: IDDSI Resources
- Don’t forget to register on www.IDDSI.org so that you will receive all the latest updates.
- Go to your App Store and download the free IDDSI App. You can use this anywhere without using data or wifi.
Creative Commons Attribution Sharealike 4.0 License. The International Dysphagia Diet Standardisation Initiative 2016 @https://iddsi.org/resources/framework/. Cannot alter beyond language translations (which are underway).
Let’s Hear From One Early Adopter of the IDDSI Framework
My questions are in purple. Bradley’s answers are under each question as follows:
1. What was the catalyst(s) or motivation(s) that lead your team at your facility to be early users?
As an Acute Care facility we discharge patients to numerous long term care facilities and rehabilitation centers, and there is different dysphagia diet terminology in place at all of them. Local SLPs at these centers even had to create a great big chart that allowed our diet terminology to be mutually understandable, so that patients didn’t fall through the cracks. This was a work-around if ever there was one!
2. Did you have a particular person (champion) outside your speech-language pathology department that helped the new IDDSI framework move forward quickly?
Absolutely – especially the Director of Support Services and the Manager of Food Services – those with direct accountability for the kitchen and diet office. In the case of the way we implemented IDDSI, unusually the executive/corporate leadership commitment on this quality project was not as important as the grass roots effort. This, for us, was a front-line and very shared initiative. Dietitians and the Dietitian Council were also crucial.
3. What communication challenges did you have around diet and liquid labels before IDDSI? (i.e., did people have difficulty knowing the difference between nectar and honey, did doctors use the ambiguous term of “mechanical soft” even when this was not an official diet order, did doctors think they were getting a pureed diet when they ordered “Soft”?)
We didn’t have a Nectar/Mildly Thickened consistency before, but we do now, thanks to IDDSI. We had all of the other above issues you mentioned.
4. How was your tray accuracy prior to IDDSI, and have you started looking at tray accuracy now after IDDSI?
We have yet to pull the data as we have not completed a full review of “Soft & Bite-Sized” diet items, so we are not yet compliant with the complete IDDSI framework.
We do now have an agreed process and flow chart for when items on a tray are not appropriate to the prescribed diet, and when and how they get reported on our safety incident system, or alternatively when they are reviewed with the Diet Office. The IDDSI initiative has also caused us to review and be very deliberate and consistent about how we identify safety incidents.
5. How are you labeling the diets and the liquids now? Have you fully adopted the IDDSI Framework labels? (I broke some questions down into parts.)
- Dual labeling is coming soon from industry.
YAY!!! We can’t wait – the industry labeling will be the sustainability of this work.
- Are you dual labeling in your recommendations/orders for diets and liquids, (e.g., with “nectar, aka mildly thick” or “ground, aka minced & moist”)?
Actually dual labeling is what has allowed us to move forward without increasing patient risk of harm by confusing terminology unknown to other team members. We have dual labelled our Diet Orders, Diet Sheets, documentation, and, deliberately, orally (as much as we can remember to).
The titles can be lengthy, but over time and with repetition, it will be possible to drop the local language. As long as our bought-in products are dual labelled, we will be dual labeling in our orders and diet sheet. Years down the road we will drop the old local labels and no one, at that point, will care, and patient safety will have been completely unaffected through the process.
- Are you using mainly the label or also the number and color system that goes with the IDDSI framework and descriptors?
We are using the labels at this time. We would use IDDSI colour if colour was an option for a particular need, but we have to focused on the language. As I think of it now, when we no longer dual label we will probably ramp up the use of colour and number, as the redundancy of the information can only help.
6. How has your kitchen changed dysphagia diets to be in line with the dysphagia diet descriptors (definitions according to the IDDSI framework)?
- Is your kitchen preparing pureed foods any differently, to make sure the texture is truly smooth and moist?
No real change needed here with our purees.
- Is your kitchen able to follow the 4mm particle size for the Minced & Moist diet?
We did not ask initially for a lot of change from the kitchen, but we first tested all food items where there had been concerns identified. Then, we tested all the foods in the Minced & Moist diet for compliance. We dropped those that were not compliant and then made plans for compliant replacements for the gaps that were created. In some cases the replacement plan was buying in a pre-made diet item, in others it was dropping the item (e.g., bananas). In other cases, like with tinned/canned fruit, we changed to a different brand. Another example was with rice, and now our own kitchen prepares it differently.
- Is your kitchen adding extra sauces to the tray for Minced & Moist?
No, although they are only serving particular food items that already have gravy or sauces. The item is specified on the diet sheet as with gravy/sauce and to serve only with the gravy/sauce.
- Is your kitchen able to follow the 1.5 x 1.5 bite size for the Soft & Bite-Sized diet?
Soft & Bite-Sized, our last frontier!! We didn’t do everything at once.
First, we added Mildly Thickened Liquid to the full range of liquid consistencies.
Then Puree was evaluated by a quick internal SLP review, and no significant concerns were found. However, this may be tweaked down the road.
Third, we addressed Minced & Moist with a full active engagement of kitchen staff, dietitians, and SLPs. We focused on concerns, performed testing, found gaps, and implemented plans, as noted above.
Soft & Bite-Sized, I anticipate, will be same process as Minced & Moist.
Finally, we will revisit Puree as a culmination – all in good time – and will cycle back and revisit as incidents and good practice suggest is needed.
- For regular food items that happen to be soft and cohesive, like lasagna or shepherd’s pie, is your kitchen leaving these whole for the Soft & Bite-Sized diet?
Stay tuned.
7. Have you had challenges with foods like bread or mixed-consistencies? Are these allowed still, and if so, on which diets? (or in a case-by-case basis per the evaluating SLP?)
Bread….yes ….especially since the modified diets may be used in particular cases. For example, when a person is edentulous, staff (mostly dietitians) may downgrade the person’s diet for reasons other than difficulty swallowing. So we actually have agreed to a non-IDDSI standard diet option which is Minced with Bread. The clinician can still expect that the typical Minced & Moist is IDDSI compliant, while this particular variation of Minced with bread is known as only a variation. Bread just opens so many options and in the world that is also trying to manage high levels of malnutrition (44% in acute care hospitals); therefore, we added this frequently used variation.
We are really trying not to add non-IDDSI standard diet options for dysphagia. Hopefully Minced with Bread will be the only one. Our electronic diet order system allows specific additions to be made (and extracted) on a case-by-case basis. This allows, for example, the patient with both renal needs and dysphagic needs to have SLP-tested safe additions. Clearly this requires effective coordination by the SLP with dietitians, nursing, the kitchen, etc.
8. Do you think you will add slightly thick liquids as an option at your hospital? (for pediatrics and adults?)
We don’t currently have any plans to do so.
9. Are the speech-language pathologists starting to modify what they test during an instrumental exam, given IDDSI findings about the challenges of mixed-consistencies and the increased choking risks on breads?
Our clinicians use MBSImP protocol during an instrumental assessment, so I couldn’t speak to this.
10. Please highlight some of your successes and your challenges. Please include ideas for how to overcome some of the challenges in your early implementation of the IDDSI framework.
Our videofluoroscopic swallow study barium recipes have been IDDSI tested and posted (SLP student project). NOTE: Canada does not have access to Varibar barium by Bracco. Recipes can be found on Dr Steele’s website (www.SteeleSwallowingLab.ca) at Best Practice – Barium Recipes. See also this article: Mapping Bracco’s Varibar® barium products to the IDDSI Framework by Catriona M. Steele, Ph.D. (2017).
Dietitians have performed IDDSI Flow Tests (see IDDSI Testing Method document and IDDSI Flow Test Poster) on their oral nutritional supplements and identified concerns. Both efforts were spontaneously generated projects from these groups which attached themselves to the IDDSI work.
Early challenges were actually in the opportunity to make the project take hold. As with every large hospital, we have ongoing challenges and opportunities. For example, issues with no Nectar/Mildy Thick consistency, diet incidents, and concerns about particular foods which were frontline generated. We started addressing these concerns and made the solutions IDDSI compliant. For example, when introducing a “nectar” consistency, let’s not call it nectar from the outset – lets introduce IDDSI testing methods with the new mildly thickened option.)
We are moving steadily forward, embedding a way of thinking, as well as a consistency and standardization of practice. Each time we take a step forward we know we are embracing more order, less inconsistency. There is really no downside.
While completely eliminating dysphagia diet related problems may be unrealistic, we are always striving to enhance the care we provide; in this case, by using IDDSI process, framework, descriptors, and language. We are using only IDDSI written language (paired with the old language), and all but the Soft & Bite-Sized diet have tested as compliant.
Thank you to Kim Bradley and her entire team at St Michael’s Hospital in Toronto, Canada for paving the way and showing us how to raise awareness, prepare our facilities, and adopt a new system using the IDDSI Framework. It is clear that this is best for patient safety by standardizing our care that we provide to patients with difficulty swallowing (dysphagia).
Please share you thoughts, questions, and findings as you and your facility progress through the IDDSI’s stages of Aware-Prepare-Adopt.