
Diet Safety: Terminology & Definitions Matters!
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com (updated 2024 with IDDSI’s new website links)
This blog was inspired by my own frustrations with different non-standardized diet names across different institutions all around the nation and the world. Dysphagia ground, mechanically altered, mechanical soft, and chopped really mean the same thing? How can we ensure diet safety when the labels and definitions are so vague? People are dying from choking events due to facilities not adopting standardized terminology and testing methods!
This blog was also based on the following session at the ASHA convention in 2014:
Steele, C. (2014, November). 1038: Diet Texture Terminology: Establishing an International Consensus. Seminar presented at the annual convention of the American Speech-Language-Hearing Association, Orlando, FL.
Steele’s work was a collaboration by the international group of volunteer researchers, clinicians and scientists: IDDSI: International Dysphagia Diet Standardisation Initiative (www.iddsi.org)

Is this meal safe?
Introduction to diet safety
Diet safety is one of the most serious patient safety issues in our field, not to mention the impact on the patient’s quality of life. I have heard doctors order “soft” diets when they think they are ordering a pureed texture.
There have been sentinel events due to a patient receiving the wrong diet.
Sentinel Event: an unexpected patient safety event that results in death, permanent harm, or severe temporary harm (per the Joint Commission).
www.jointcommission.org/sentinel_event.aspx. Joint Commission calls adverse events “sentinel” because “they signal the need for immediate investigation and response.”
We have to be proactive members of the healthcare team to prevent errors in diet orders and meal tray inaccuracies.
However, how do we do this when there is so much confusion between the labels for solids and liquids? Steele noted: “no clear agreed upon taxonomy causes a clear risk to our patients.” Steele referred to the 1996 ADA Convention when 71 dietitians from 27 states responded to a survey about diet textures. They had 40 different labels for solid food textures and 18 different names for liquid viscosities!
Standardization is clearly needed.
What do we do when even the literature does not agree with practice?
Steele pointed out that Protocol 201 by Logemann, et al. (2008) & Robbins, et al. (2008) used 300 cps for Nectar thick and 3,000 cps for Honey thick. (Note: cps is also written as cP or centipoise, and this is the same as mPa.s or millipascal.) One of the conclusions of Protocol 201 was that patients on “honey-thick liquid” had poorer outcomes than patients on nectar-thick liquid. However, honey-thick liquid, per the National Dysphagia Diet’s recommended ranges, is at a viscosity of 351 to 1750 cps. The honey thick Varibar product we now use for Modified Barium SwallowStudy.com is labeled at 1500 cps. (Per Bracco website regarding Varibar: “Thin Honey” EZ-EM #D121, has a measurement range of 800-1800 cps; whereas, “Varibar Honey” used in Protocol 201 measures between 2500-3500 cps). Was Protocol 201 really comparing Nectar thick to an almost Pudding thick liquid? This research has changed how we practice, making us want to recommend nectar thick liquid much more often than honey thick liquids. Was this shift in thinking based on research that tested with a honey consistency that was too thick?
Questions to ask ourselves during our evaluations:
Are we modifying the diet due oral factors or pharyngeal issues that we cannot see at the bedside? Are we modifying the diet based on physiological problems that we saw on an instrumental evaluation? Regular solids take more effort to chew, may cause fatigue, and may cause choking if the bolus is swallowed before adequate mastication and oral preparation to make the bolus swallow ready. Therefore, some diet modifications may be helpful, but “there is very little literature specifically about texture modified food used for the management of dysphagia,” per Steele.
According to Steele, there is evidence in literature that thickening liquid can help prevent aspiration of a thin liquid, but there is also evidence that there is a level that is “too thick.” There is also evidence that when technicians thicken by sight, the liquid tends to be thicker than the target. If we thicken the bolus too much, and the patient has significant pharyngeal dysphagia, are we causing increased pharyngeal residue? We do not know the answer to this question if we are recommending a thickened liquid based on a bedside swallowing evaluation without an instrumental exam.
Some pureed textures may also be too thick and sticky. Steele noted that if we adequately masticate and prepare a solid bolus until it is “swallow-ready,” what we send to the pharynx is quite similar in texture to a puree. (The exception is bread – keep reading.) I once had a patient in her 90’s who had significant trouble clearing a pureed bolus through her upper esophageal sphincter (UES) due to a chronic cricopharyngeal dysfunction; she said she would be the blender instead and pulverize the food in her mouth. This strategy plus her piecemeal swallows worked better than a pureed bolus swallowed all at once. However, we will not know what truly works unless we see it in action using an instrumental swallowing evaluation.
More questions related to diet safety…
- Should oatmeal really be on a pureed diet? It can be a mixed consistency at times.
- Is Germany really using 3D printing to make molded purees?
- Are all molded purees really a smooth pureed texture?
- Should we really be pureeing bread into a sticky glob?
- How do we test purees to answer this question? (See IDDSI Testing Methods with the Spoon Tilt Test).
- Should we allow bread on any dysphagia diet? Steele noted that the food-oral processing literature found that we send bread to the pharynx at a less processed state than other solids. We try to swallow it before it is swallow-ready. If the mouth is dry, bread may be extra difficult. Saliva adds the amylase enzyme to break down the starches in bread.
- What does amylase do to thickened liquids? It may destroy the starch-based thickeners, so how do we know the patient is swallowing the appropriate viscosity?
- Do some liquids thicken differently? Garcia, et al (2005) found orange juice thickens faster than water, apple juice, and coffee. Thickened whole milk is actually not as thick as thickened skim milk; the milk fat actually interferes with the bonding of the starch thickener. The gum thickeners may be promising, but have problems too. Per Steele, manufacturer recipes for gum thickeners do not seem to reach the same viscosity ranges as the comparable recipes for starch.

Is this a Honey-Thick Liquid?
And what about shear rates with LIQUIDS?
The shear stress that our tongue applies to a liquid bolus as it strips across the hard palate is a shearing force across the top of the bolus. The yield stress is how hard you have to push to get the flow to start. We apply pressure and cause deformation (which can change the shape of the bolus and make it spread out). The shear rate is the change of velocity as one layer of fluid passes over an adjacent fixed layer. The shear rate is noted in “reciprocal seconds” [1/s or s-1 suprascript].
This get’s a bit deep into Rheology. This is why we need Materials Science collaborators.
Here is a bit of what Steele discussed at the session:
She explained how there are zones in liquids that flow differently; for example, the liquid will meet resistance along the pharyngeal walls but flow faster in the center of the bolus. Liquid also moves slower when it is in a cup versus when it is being swallowed. Shear rates speed up off the tongue.
The flow characteristics really change when we start modifying them. Our blended smoothie may appear to be honey thick, but it can change to a thin liquid over time. We need to know if the fluid is a Newtonian or a Non-Newtonian fluid. Water is assumed to be Newtonian, but no fluid really fits this perfect mathematical model. Newtonian fluids would have a constant viscosity that does not depend on the stress or velocity. Many fluids we give to patients are non-Newtonian, and that is where our diet modifications get very tricky. For example, ketchup is a non-Newtonian fluid, as it becomes thinner at higher shear rates.

Ketchup is a Non-Newtonian Fluid
Another example of a non-Newtonian fluid is a thickened liquid. Non-Newtonian fluids have “shear-thinning” characteristics, meaning they thin under stress and changing velocity. Steele showed a chart of various pre-thickened liquids with apparent starting viscosities of nectar thick, honey thick, and pudding thick (aka, spoon thick or custard thick). All of the liquids thinned as the shear rates increased. The pudding thick liquid supplement stayed a pudding thick liquid when in a cup. However, it thinned to a honey thick liquid at shear rates just over 50/s-1. Shockingly, that pudding thick liquid thinned to a nectar thick liquid at faster shear rates of 500-1000/s-1. Steele cited Withers et al. (2013) when noting that shear rates reach 400/s-1 through the pharyngeal and esophageal stages of the swallow, per computer simulations with water.
The bottom line, per Steele, is “we cannot compare the apparent viscosities of liquids that are quoted at different shear rates.” We cannot even compare Varibar Barium (with it’s reported viscosities at shear rates of 30 s-1) to other liquids the patient may consume. Steele noted that when Varibar Thin Barium is reconstituted to 40% it may actually be thicker (i.e., 10 mPa.s) versus water at 1 mPa.s. Are we getting false negatives on the Modified Barium SwallowStudy.com?
What diet safety factors should I consider with SOLIDS?
Is the bolus moist and cohesive or does it fracture under force?
Steele introduced a new term for me: Tribology. Thanks to Wikipedia, I am understanding this more. This materials science perspective makes a lot of sense for our analysis of solid textures and mastication. We are talking about spit and slipperiness, per Steele. This is the science of how surfaces interact in motion, using principles of friction (including adhesion and cohesion), lubrication, and wear. The wear (or effort of chewing) can be minimized by modifying the surface of properties of solids through the use of lubricants (per Wikipedia.org/wiki/tribology fundamentals).
SLP’s need to be aware of the science behind our dietary modifications when treating patients with dysphagia.
We need to know why we are recommending modifications.
We need to know that what we recommend has been standardized and analyzed thoroughly.
Not to mention, we need to thoroughly assess mastication and food oral processing.
National Dysphagia Diet (NDD)
The NDD was a project of the ADA with assistance from Speech-Language Pathologists and a food scientist (rheologist), but ASHA was not an official partner and never gave their support to NDD (ASHA has fully supported IDDSI and implementation across the US and Canada started in 2019). In my opinion, the NDD was the best thing out there at that time. See “IDDSI replaces NDD” on SwallowStudy.com under Dysphagia Resources and Patient Handouts on what IDDSI Diets have replaced the following NDD diets: Dysphagia Advanced, Dysphagia Mechanically Altered/Dysphagia Ground, and Dysphagia Puree.
HOWEVER, the NDD was meant to be a start, but the tweaking of the NDD has not happened yet, per Steele.
There is HOPE, but it will take a global village!
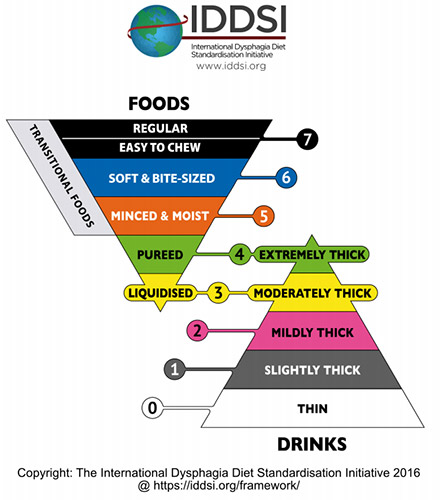
Dr Catriona Steele, from Toronto, and many others from around the world are advocating for an international consensus approach. They created IDDSI: International Dysphagia Diet Standardisation Initiative (www.iddsi.org) to standardize food and liquid levels. You can tell it is global with the different spelling of standardization!
Another goal of IDDSI is to choose labels that do not have implied meaning and are culturally sensitive. For example, I once had a doctor ask why I was suggesting to add “honey” to the diabetic patient’s liquid.
See IDDSI website and the group’s work so far in the Open Access Publications/pdf‘s below:
A global consensus, based on evidence, is coming soon.
Minimize risks for our patients.
End the diet texture modification guesswork.
And maybe answer a few of the food science questions!
2016 Updates:
- See blog: “No Dysphagia Diet Modification Without Standardization!”
- Follow @IDDSI_org on Twitter for updates
- The framework is complete and under the Creative Commons for all to use!
- Download your FREE APP from your app store by searching “IDDSI” – once downloaded it operates without Wifi. Has videos to teach your patients how to test the thickness of liquids with the easy Flow Test.
- Did you know that the diets and liquids were labeled with simple language that can be easily translated? The framework is already translated into over 16 languages. NO MORE “Nectar” and “Honey.” These are now “mildly thick” and “moderately thick,” respectively, and many of the thickener companies are already on board with these changes and preparing to change packaging. See www.iddsi.org for all details.
2024 Updates:
References cited from Steele’s session:
Garcia, J.M., Chambers IV, E., Matta, Z. & Clark, M. (2005). Viscosity measurements of nectar- and honey-thick liquids: Product, Liquid, and Time Comparisons. Dysphagia, 20, 325-335.
Withers, C., Gosney, M.A. & Methven, L. (2013). Perception of thickness, mouth coating and mouth drying of dairy beverages by younger and older volunteers. Journal of Sensory Studies, 28 (3), 230-237.
This was great info.
My husband had throat cancer in lymph nodes in 2003. Due to radiation his throat has progressively narrowed and he has acute chronic aspiration pneumonia. A speech therapist is working with him. He has lost about 12 lbs. We are trying to figure out his food intake and thicknesses that he can eat without food going to lungs. It is a challenge.
He doesnot want a pic line.only as last resort
We are now working with ENT at MDAnderson in Houston Med Center
He is also being treated for container prostate cancer with radiation. All challenges. Main concern is food intake which I am at a loss. We are just trying different foods and thicknesses. Trying to decide if plain water is the worst for aspirating.
Thank you again for your articles and studies.
This was great info.
My husband had throat cancer in lymph nodes in 2003. Due to radiation his throat has progressively narrowed and he has acute chronic aspiration pneumonia. A speech therapist is working with him. He has lost about 12 lbs. We are trying to figure out his food intake and thicknesses that he can eat without food going to lungs. It is a challenge.
He doesnot want a pic line.only as last resort
We are now working with ENT at MDAnderson in Houston Med Center
He is also being treated for contained prostate cancer with radiation. All challenges. Main concern is food intake which I am at a loss. We are just trying different foods and thicknesses. Trying to decide if plain water is the worst for aspirating.
Thank you again for your articles and studies.
Hello all:
I responded directly to this inquiry, but I thought I would share a summary to help more individuals.
I am so glad that you are working with swallow specialists (speech pathologist/SLPs who specialize in swallowing) at MD Anderson! Kate Hutcheson, from MD Anderson, has pioneered our evaluations and treatments for people with radiation-associated dysphagia (RAD), as they call it. They can help him work back up the ladder (or pyramid in the case of the IDDSI diet framework) of eating more and more challenging food in a safe way. Eating and swallowing food is exercise. The ball of food is like lifting weights. Important concept: “use it or loose it,” but the SLP has to help guide was is safe at each time point in recovery. Initially, as dysphagia becomes more severe after radiation, thicker liquids and very moist purees may be needed, but they can test that with a video swallow study (VFSS, aka, MBSS) or endoscopic swallow study (FEES).
1. See also this blog:
https://swallowstudy.com/tips-survivors-head-neck-cancer/
Keeping mouth clean and moist are essential parts of eating, as well as pain management coordinated with mealtimes. There are some tips there, but your SLP and team will provide more handouts of tips to make eating easier and less painful.
2. See also:
this article I wrote for Hormel Health Labs:
https://www.hormelhealthlabs.com/resources/tips-for-managing-dysphagia-at-home-during-the-holidays/
* See also my “news” section about this Hormel Health Labs article. I have more links to handouts about how to make pureed foods. See also EssentialPuree.com by Diane Wolff.
3. Regarding your question about what is “worse” for aspirating. Thin liquids (water included) are the most common consistencies to be aspirated; however, if it is just plain water with a very clean mouth and oral through pharyngeal/throat cavities, that water may be fairly benign on the lungs if aspirated. We call that a “Free Water Protocol,” which is allowing clear water between meals, even when a person may require diet and liquid modifications (e.g., thickened liquids) to be safer during a meal.
For a good review of free water (only water) between meals. See: Why I Like the Free Water Protocol, by
Dr. Susan E. Langmore, https://doi.org/10.1044/sasd20.4.116
Main point: Only with a clean mouth (i.e., using electric toothbrush/toothpaste and mouthwash are best – alcohol free, and flossing if he can), would someone be “safer” to drink water and have some aspiration get into lungs without a high risk to develop aspiration pneumonia or other negative consequences. The idea is that water is benign if it hits the lungs without all the bacteria, other pathogens, sugars, acids, and more. HOWEVER, first review with SLP AND DOCTOR AT MDANDERSON. please don’t try this on your own without making sure that he is a good candidate. Underlying lung complications may make him not a candidate for small aspirations of water and/or if he can’t clean his mouth well due to pain.
Hope that all helps.
Any advice should be reviewed with his medical team as ai have not reviewed his case. This is general info providing only and cannot substitute for direct care.