
Patient Safety: Transitional Foods (Part 2)
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com

Introduction to Part 2 of Transitional Foods
Welcome back to Part 2 of my 3-part article on Transitional Foods (in the dysphagia diet framework on www.IDDSI.org). In Part 1 of this blog series, I addressed what transitional foods are, how to test them, ideas on their use in dysphagia treatment, and an example of a transitional food product.
Next, it is important to address potential choking risks when working with people who have difficulty swallowing, as well as when feeding the very young and the geriatric populations. Just because products are marketed to a baby to toddler age group, does not mean that they are safe.
Again, with my disclosures: I am not receiving any financial incentive to mention specific products. Additionally, when I say: “patient safety,” I am referring to safety of all people – babies through geriatric population. The term “patient safety” is a key phrase in healthcare, for good reason!
In this article, I will:
- Review the definition and statistics around choking.
- Discuss the dangers with some products that may be marketed as transitional foods for children through geriatrics (also known as first finger foods for babies and toddlers). I like to call them “transitional food imposters.”
The future Part 3 will cover:
- Japanese Konjac Jelly (aka, Konjac Candy or Konnyaku) that has been taken off the market in the US by the FDA due to choking events.
- Transitional foods that are extra challenging for people with dysphagia (e.g., gelatin or Jell-O).
- Transitional food items (training jellies) that are used in dysphagia treatment in Japan and how these are different from the Konjac Jelly.
Choking & Patient Safety
Thousands of people die each year from preventable choking-related injuries. In the year 2016 in the US, over 100 children under the age of 4 died from choking. The incidence of choking starts to sharply increase in adults after the age of 55 and really peaks when people are in their 80’s. The CDC found that unintentional injuries were the 4th leading cause of death, and choking is in that large category.
By the way, these numbers do not even include deaths due to aspiration of foods and liquids. The CDC reported 19,803 deaths in 2015 caused by pneumonia/pneumonitis due to solids and liquids. (More on the difference between actual choking and aspiration in the next section.)

For patient safety, it is important to recognize the universal sign of choking, which is the hands up around the neck.
Very young toddlers, bedridden elders with limited mobility and communication, and people with difficulty swallowing may have altered sensation and minimal ability to show that they are choking. They may not give you that typical hands to the neck universal choking sign. Therefore, these at-risk populations need to be carefully supervised during the entire duration of snack-time and meal-time.
Transitional Foods & Patient Safety:
True Transitional Foods that have passed the IDDSI Testing Methods, which were described in Part 1, will not likely cause choking. The food item should have dissolved or melted down to not block the airway. However, don’t believe the packaging. Parents and caregivers need to test these foods for themselves.
Side-note & Crucial Clarifications on Choking versus Aspiration:
Many people use the term choking too loosely. People say, “my toddler choked,” when he may have just gagged on a piece that was too large for his mouth.” Good thing he gagged to eject that huge bite out of the mouth before it reached the throat. That is your warning sign to supervise smaller bites. Some people complain of “choking,” when in fact they are coughing on food particles and/or liquids go down the wrong way but do not actually block off the airway. Material poking into the top of the airway (or laryngeal vestibule/voice box) is called penetration. When the material drops below the level of the vocal cords into the trachea and lungs, that is called aspiration. Aspiration can happen silently when material drops down the wrong way and there are no outward signs of coughing or throat clearing. Silent aspiration is quite common in the elderly who are sick and deconditioned. Silent aspiration is also common when people who are critically ill. Many issues can cause reduced sensation in the airway, such as: some medications, intubation, and diseases/conditions that decrease the sensation to the throat and airway (e.g., Parkinson’s Disease, Dementia, radiation therapy to the head/neck, and even Chronic Obstructive Pulmonary Disease or COPD).
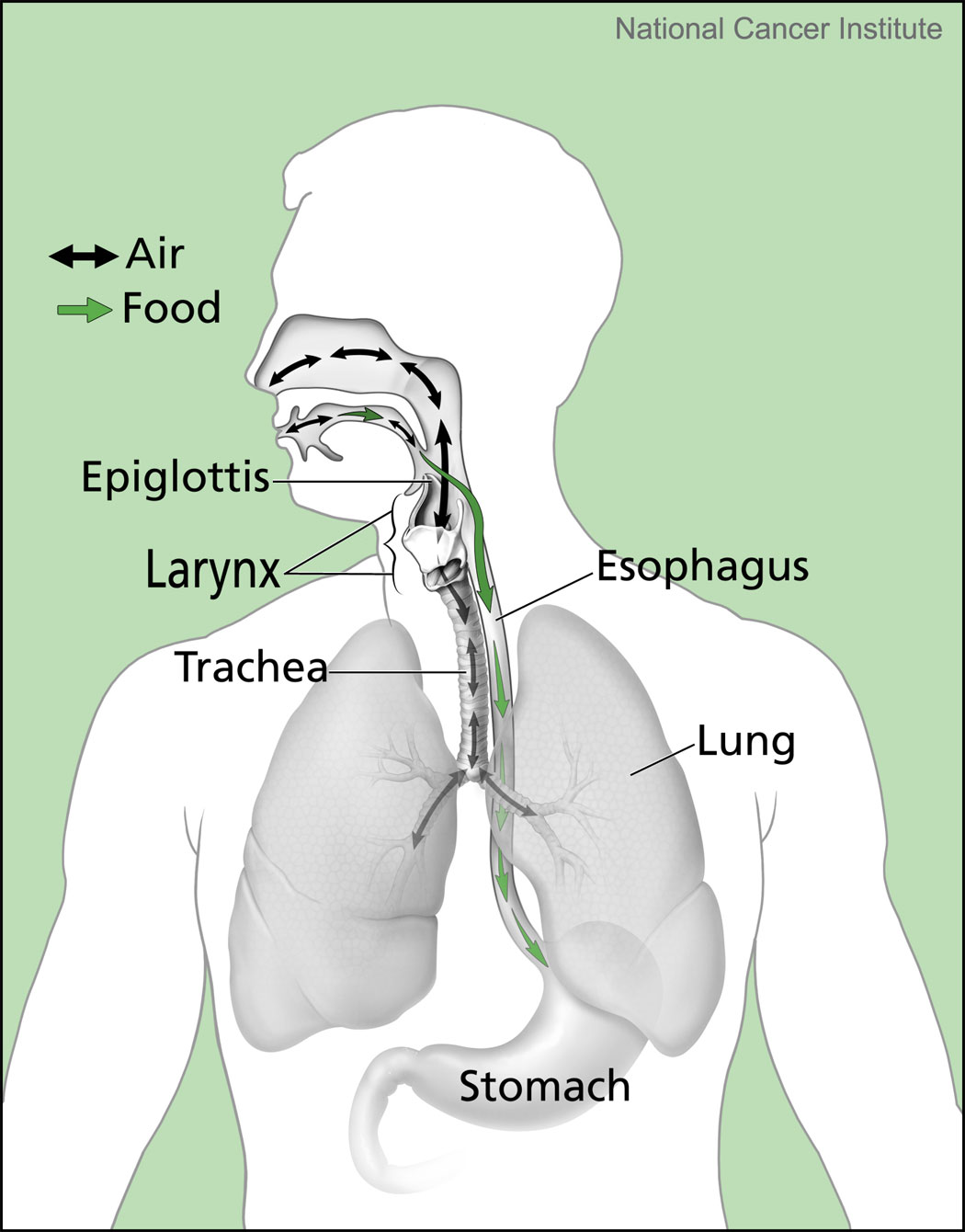
Choking is caused by an actual airway obstruction when food or an object blocks your entire lower throat area and/or the opening to the airway, which is your larynx (aka, voice box or where you feel your “Adam’s apple”). Your larynx or laryngeal vestibule sits at the top of the trachea, which is the tube leading to the lungs. (It is pretty crazy that we breathe and talk out of this same hole. A hole which has to close off to safely swallow.)
When someone is choking, she/he may show the universal sign of choking, which is clenching the hands around the neck. However, choking may happen without initial audible gasping, coughing or any significant obvious signs. A piece of food or an object may suddenly become stuck in the airway. In young children and in the elderly, you may not see any initial distress until you realize that the person is not be able to breathe in or out. If you do see strong coughing, that is good; encourage that. If no airflow or very little airflow is detected, then it is likely choking and airway blockage. You may see the person’s face change to red and then even get blue around the lips. You may only have a minute or two before the person becomes unconscious. If you or a loved one is at risk for choking (especially if you have a new baby or live or work with the elderly), learn the Heimlich Maneuver now. The American Heart Association is on example of how to find a course near you.
What increases choking risks in young children?
(Awadalla, et al., 2018)
- Dentition: young children do not have posterior dentition necessary to grind tough foods.
- They lack mature rotary chewing skills.
- They lack tongue lateralization to move the food to the molars for chewing and to maintain control of the food in the mouth.
- They have front teeth that can bite off a big piece but lack the other skills to manage it.
- They have poor oral control and coordination.
- They have poor safety awareness and may engage in running, playing, laughing, yelling and/or talking with food in the mouth.
- They are impulsive and may have dangerous eating behaviors, like shoveling or stuffing food into their mouth in large bites/mouthfuls.
- The anatomy is different in an infant and toddler, with more narrow airways and the larynx and airway is higher in the neck, right behind the tongue base.
Isn’t it interesting that many of these reasons for choking (except for #8) can be applied to other populations of people at risk for choking (e.g., people who have had strokes; the frail elderly; people with cognitive impairment, traumatic brain injury and dementia; people with mental illnesses; and people with developmental disabilities – to name a few).
All that said, if choking is at all a risk, the bite-sized pieces of a transitional food could be presented in 1.5cm size bites for adults and 8mm size bites for children, per IDDSI. (Keep in mind the average adult male airway is 21.5mm and the average adult female airway is 17mm. Whereas the average pediatric airway is 8mm and the infant airway is 6.5mm.) Bite-sizes larger than these measurements would pose a greater choking risk.
Transitional Foods & First Finger Foods
The American Academy of Pediatrics (AAP) recommends that children can start these first finger foods (transitional foods) when they can:
- Sit up without support and
- Bring their hands to their mouth, which usually is around
- 9 months (with wide variability).
It was great to see that Awadalla and colleagues (2018) stressed the importance of introducing a varied diet of early finger foods by 10 months (for typically developing infants) in order for infants to gain important oral-motor skills that are precursors to chewing (Awadalla and colleagues cited research by Delany & Arvedson, 2008).
However, buyer-beware!
Test your transitional food or first finger food item for patient safety
We are all told that hot dogs, grapes, raw carrots, hard candy and small toys are major chokables. However, when a product is specifically marketed to your baby, how are you to know that it could cause choking?! Since many products do not have rigorous testing standards, you need to be the food tester before you give something new to your loved one (this applies to babies through geriatrics).
AAP recommends that first finger foods should be:
- Soft,
- Easy to swallow, and
- Cut into small pieces.
That is a little too general, right?
Fortunately, you can test the items yourself and analyze them for safety as discussed in Part 1.
Testing Transitional Foods & Finger Foods = Increased Safety
Awadalla and colleagues (2018) did testing for the consumer. Their research turned 41 members of the pediatric team at Cohen Children’s Medical Center of New York into food testers. They examined 9 products marketed as appropriate for first finger foods. These products were General Mills Cheerios and 8 items from Gerber (Fruit and Veggie Melts, Yogurt Melts, Apple Pickups, Carrot Pickups, Lil’ Crunchies, Wagon Wheels, Arrowroot Cookies, and Puffs). All items were tested “fresh” out of the box and “exposed” after being left out for one hour. (How about after being in the diaper bag all day!)
Testers were told to dissolve the items in the mouth without using teeth. They recorded the time each item took to “become soft and break up” and “dissolve completely or become small enough that it had to be swallowed (p891).” Researchers found that only the Apple Pick-ups and Carrot Pick-ups met the AAP recommendations (that is only 2 out of 9 products). Note: As of April 2022, I do not even see these “Pick-ups” products still on the market per a quick online search. All the other items failed on softness, which is why we also need to test how fast they dissolve. Many products became soft within seconds and most products dissolved without chewing in 10-25 seconds for fresh and exposed. This is certainly a good benchmark to look for when you are doing your own testing. Cheerios, Puffs, Lil’ Crunchies and the Pick-ups dissolved in less than 15 seconds.
However, the Gerber Fruit and Veggie Melts completely failed and should be taken off the market (and maybe they have according to my search on Gerber’s website). Testers noted that the Fruit and Veggie Melts formed a small-hard ball and dissolved in 36 seconds on average when fresh. When exposed, they took up to 1 minute to dissolve and were described as “marshmallow-like,” “like a hard candy,” which could block an airway. Hard candy is a very common item that causes non-fatal and fatal choking events.
Gerber Arrowroot Cookies and Wagon Wheels are labeled “graduates,” but if Gerber considers these for an older child, than maybe they should take that cute little baby logo face off the package. It makes you think they are for 6-9 month olds. Testers found them to be way too big for one bite and not appropriate for first finger foods. These items were scratching the roof of the testers’ mouths when waiting for them to dissolve. Therefore, the Arrowroot Cookies and Wagon Wheels were also epic fails when it comes to our transitional food testing and AAP recommendations for first finger foods for babies under 10 months old. The Wagon Wheels were described as not easy to swallow, too big and not soft. Lil’ Crunchies are also not infant bite-sized and not soft. Researchers warned that toddlers with front teeth can bite off way too big of a piece with the inability to break it down.
My go-to teething wafer for my son was Baby Mum Mums, which may work as a teether, but new research has now showed that their dissolvability is quite poor, especially when the person has dry mouth and/or dysphagia (Barewal et al., 2021). Therefore, Baby Mum Mums are not a good transitional food item for dysphagia management, whereas the product Savorease with all the crackers and dips are good transitional food items for the rehabilitation of chewing and oral preparatory skills (Barewal et al., 2021). Read more here.
Bottom Lines on patient safety and swallowing safety:
- Play with the food before your child (or loved one with dysphagia) does. Test it, as noted in Part 1.
- Keep all transitional foods in air-tight-sealed containers to maintain freshness and prevent a marshmallow-like consistency from forming, and
- Supervise all at risk individuals at snack and meal-time.
*******
Go to Part 3 of this 3-Part Series on Transitional Foods.
Patient Safety/Transitional Foods References
Awadalla, N., Pham, T. & Milanaik, R. (2018). Chew on this: Not all first finger foods are created equal. Clinical Pediatrics, 57(8), 889-894. https://www.ncbi.nlm.nih.gov/pubmed/28990427
Delany, A.L. & Arvedson, J.C. (2008). Development of swallowing and feeding: Prenatal through first year of life. Dev Disabil Res Rev, 14, 105-117. Doi: 10.1002/ddrr.16. https://www.ncbi.nlm.nih.gov/pubmed/18646020
New Reference on Transitional Foods:
Barewal, R., Shune, S., Ball, J. et al. (2021). A Comparison of Behavior of Transitional-State Foods Under Varying Oral Conditions. Dysphagia, 36, 316-324. https://link.springer.com/article/10.1007/s00455-020-10135-w
This author has nothing to financially disclose regarding the products mentioned in this article.