
Hidden Struggle: 7 Updates in Dysphagia from Head and Neck Cancer
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction to Dysphagia in Head and Neck Cancer
June is Dysphagia Awareness Month, and we continue to uncover challenges that people experience when they have difficulty swallowing (dysphagia). Our first dysphagia awareness month article discussed dysphagia in general, then we reviewed neurogenic dysphagia, followed by esophageal dysphagia. Now, we need to uncover the hidden struggle of survivors of head and neck cancer. Many go through significant changes in their swallowing during and even well after treatments for head and neck cancer.
Globally, head and neck cancers represent a major health burden, ranked as the seventh most common cancer worldwide, according to GLOBOCAN 2022 (i.e., the International Agency for Research on Cancer’s database Global Cancer Observatory). Roughly 3-5% of all annual cancer cases in the United States are head and neck cancer.
One may think that cancers of the mouth, throat, and voice box are declining with people smoking and chewing less tobacco, along with more tobacco control measures in place. Many prior studies had linked tobacco smoking, tobacco chewing, and alcohol drinking to increased risks for cancer in older adults of the following areas:
- mouth (oral cancer),
- mouth to throat (oropharyngeal cancer), and
- voice box (laryngeal cancer).
However, not all head and neck cancer is due to smoking and drinking! A large-scale project out of France (Radoï et al., 2018 – ICARE) showed how a different type of cancer – salivary gland cancer – was not associated with tobacco and alcohol use at all. Rather, the ICARE project pointed to risks from industrial and occupational exposures from certain chemicals and materials.
Additionally, the Human Papillomavirus (HPV) has been on the rise and now poses a high risk for the development of HPV+ cancer of the oropharynx, which may strike in younger people (i.e., rarely in those in their 20’s to 30’s and more common in ages 40-60 years old). Fortunately, HPV+ cancers have better overall survival rates than non-HPV cancers, but we need to raise awareness to make sure these are caught and treated early on.
There are many socioeconomic disparities in our country and around the world, and these may delay this early identification and treatment for those with head and neck cancer. Even in the United States, the delay from first symptoms to actual diagnosis is too long. Primary care and dentistry need increased screening for earlier and more accurate detection efforts. Additionally, we need to expand national and global HPV vaccination programs. The earlier to diagnosis – the better odds of survival.
The two research articles are related to persons with dementia, but factors are similar for those with dysphagia from head and neck cancer:
- Eating and swallowing care disparities in persons with dementia: A conceptual framework, by Dr. Loy et al., 2025.
- Ready for Discharge, but Are They Ready to Go Home? Examining Neighborhood-Level Disadvantage as a Marker of the Social Exposome and the Swallowing Care Process in a Retrospective Cohort of Inpatients With Dementia, by Dr. Robison-Loy et al., 2024 (same lead author as above).
- Striving to Provide Equitable Dysphagia Care in an Inequitable World (webinar), by Drs. Roy-Faderman, Garcia & Loy, 2025
Survive & Thrive After Head and Neck Cancer
This June it is our hope that people with head and neck cancer survive and thrive. That is very challenging with significant difficulty swallowing (dysphagia). For survivors of head and neck cancer, this hidden struggle to swallow may persist long after the life-saving surgeries and chemoradiation therapies. June’s National Dysphagia Awareness Month reminds us that early identification, comprehensive dysphagia evaluations, and proactive dysphagia rehabilitation are vital steps to restoring nutrition, emotional well-being, and quality of life. Survivors of head and neck cancer fight to find and maintain a new normal.
Overview of Head and Neck Cancer
Before this blog provides 7 dysphagia updates on head and neck cancer from evaluation to treatment to quality of life, you may need more background on head and neck cancer. Therefore, please see this overview by the Cleveland Clinic, which reviews the types of head and neck cancers, risk factors, and symptoms to watch out for, such as:
- Persistent sore throat
- Radiation of pain up to the ears (with normal ear exams)
- Pain in your face, jaw, tongue, teeth
- Pain with chewing and swallowing
- Persistent voice changes with a hoarse or rough quality
- Lumps in the mouth, throat, face, or neck
- Sores or patches in your mouth that don’t go away
If you have any of these symptoms: Do not wait —> Please see an Ear, Nose, and Throat (ENT, aka Otolaryngologist) as soon as you can.
Please also see this resource from Cancer Support Community, where they remind that “community is stronger than cancer.” Here is their list of resources. Below is their introductory YouTube Video:
7 Dysphagia Updates in Head and Neck Cancer
- The HPV Epidemic: Shift in Head and Neck Cancer Demographics
- Collateral Damage: Radiation-Associated Dysphagia (RAD)
- Comprehensive Dysphagia Evaluations for Head and Neck Cancer
- High-Intensity Exercise
- Use it or Lose it: PRO-ACTIVE Therapy & EAT-RT Staircase
- Fortify the System: Cough Strength
- Holistic Care for Dysphagia from Head and Neck Cancer
1. The HPV Epidemic: Shift in Head and Neck Cancer Demographics
When we look back at the history of head and neck cancer, the traditional risk profile was clear-cut. For decades, the archetypal patient presenting with squamous cell carcinoma of the mouth or throat was an older individual, typically in their late 60s or 70s, with a heavy, lifelong history of tobacco smoking and alcohol abuse. However, as detailed in my review blog on HPV and Head and Neck Cancer, a modern epidemic has rewritten this narrative. My introductory article from 10 years ago was shared here on NFOSD as well. More resources from NFOSD will be shared in #7 below!
The widespread rise of the Human Papilloma Virus (HPV)—specifically the HPV-16 strain which is the same type as in cervical cancer—has created a distinctly new patient population. Today, individuals diagnosed with HPV-positive (HPV+) oral and oropharyngeal squamous cell carcinoma are significantly younger and frequently male, white, and non-smoking.
The good news and recommendations were well summarized by Abreu and colleagues (2025):
“HPV-positive (HPV+) tumors have demonstrated a better response to treatment and higher survival rates than HPV-negative (HPV-) tumors.”
The 5-year survival rates are up to 85% or more, compared to much less (30-35%) when the head and neck cancer is not related to HPV (Lin et al., 2013; Chen et al., 2020). The challenge, then, may be in this longevity itself! Typically a person with HPV-negative cancer may be in their 80’s. However, one with HPV+ may be 45 years old. Once they successfully defeat an oropharyngeal tumor they will live another 40 to 50 years with potentially progressive treatment toxicities, compromised swallowing, and altered quality of life.
2. Collateral Damage: Radiation-Associated Dysphagia (RAD)
Treating tumors of the oral cavity, oropharynx, pharynx, salivary ducts, and larynx, sometimes require surgery. Often, though, they are treated with aggressive chemotherapy and radiation (chemoradiation therapy or CRT). Radiation doses are targeted to the tumors, but there is collateral damage to the delicate surrounding healthy structures. The difficulty swallowing that results from chemoradiation therapy is known as Radiation-Associated Dysphagia (RAD).
As outlined in our prior article on the immediate (acute) and later effects of RAD, these radiation toxicities change and may progress across time:
A. The Acute Toxicity Phase (<90 Days Post-RT)
During and immediately following radiation, tissues undergo acute inflammation (edema) and cell death. During this time period, the person may experience:
- Oral Mucositis: Painful, raw ulcerations lining the oral cavity and pharynx, making chewing and swallowing painful and very challenging. Work with your medical team to spot treat the sores, as numbing the entire mouth and throat may make it hard to safely swallow. Compound medications to swish and swallow can be prescribed by your medical team, along with baking soda rinses and other tips noted here.
- Xerostomia: Radiation directly damages the cells of the salivary glands, resulting in a lack of saliva (follow that link to learn more about saliva). After radiation, saliva becomes thick, ropey, and highly acidic, increasing local friction and elevating perceived swallowing effort. (Again, read more saliva and dry mouth resources here).
- Odynophagia or painful swallowing: Swallowing can become intensely painful, frequently forcing people to restrict their oral intake. It is important to seek advice from your medical team for treatments and medications to reduce your pain before meals to continue trying to eat and swallow.
B. The Chronic and Late Toxicity Phase (>90 Days to 5+ Years Post-RT)
Once the acute inflammation subsides, a silent but potentially progressive phenomenon takes over: tissue fibrosis. The once soft and pliable tissues are replaced with scar tissue, hardened tissues from reduced blood flow, and nerve damage and compression due to these tissue changes. Over years, this can cause Late-Radiation Associated Dysphagia (or Late-RAD). Again, see the prior article more completely comparing early vs late toxicity phases in head and neck cancer.
Muscles lose their compliance, leading to significant difficulty swallowing due to the following (Hutcheson et al., 2008; 2013a):
- Impaired Base of Tongue Retraction: The back of the tongue may no longer make strong contact with the back wall of the throat (posterior pharyngeal wall). This affects our swallow pump or piston action needed to start a good clearing wave through the throat (pharyngeal peristalsis or stripping action) to drive a ball of food (bolus) downward through the throat and into the top of the esophagus.
- Reduced Hyolaryngeal Excursion: The structural complex of the hyoid bone and larynx becomes anchored by fibrotic tissue, preventing the upward and forward movement (hyolaryngeal excursion). This movement is needed for protecting the airway and mechanically pulling open the upper esophageal sphincter (UES). The epiglottis may also be stiff and not respond to these mechanics and pressures to flip down and close off the top of the airway.
- Swallow Safety impairments: causing food/liquid to penetrate into the top of the voice box/airway (laryngeal vestibule) above the level of the vocal cords, and potentially aspirate. Aspiration is when material drops below the vocal cords into the trachea, which goes to the lungs.
- Swallow Efficiency impairments: causing significant residue throughout the mouth, throat, and/or esophagus after the swallow, which can also put someone at risk for aspiration and choking/airway blockage after the swallow.
- Reduced Sensation & Silent Aspiration: Because radiation also destroys local sensory nerve endings, material can enter the laryngeal vestibule and drop below the vocal cords and into the lungs without triggering any protective cough response.
3. Comprehensive Dysphagia Evaluations for Head and Neck Cancer
Standardizing the Video Fluoroscopic Swallow Study Ratings: DIGESTv2
Historically, when an SLP completed a Videofluoroscopic Swallow Study (VFSS) or Modified Barium Swallow Study (MBSS) on an oncology patient, the resulting report was highly subjective. Phrases like “mild-to-moderate pooling or residue” or “trace aspiration” failed to provide quantifiable metrics that could be reliably tracked across the person’s multi-year survivorship plan of care.
To bridge this gap, Dr. Katherine A. Hutcheson and her colleagues developed the Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) criteria (now on DIGEST Version 2) (Hutcheson et al., 2017 and 2022). DIGESTv2 provides a validated, standardized tool that summarizes complex videofluoroscopic swallow study observations into a multi-dimensional severity grading system, ranging from 0 (normal) to 4 (profound).
DIGEST scores the person within two distinct grading scales:
- Safety (DIGEST Safety Grade): Quantified by the depth, quantity, frequency, and the person’s response to airway invasion, expanding upon the Penetration-Aspiration Scale (PAS).
- Efficiency (DIGEST Efficiency Grade): Quantified by the percentage, location, and persistence of post-swallow pharyngeal residue across solid and liquid trials. The clinician looks at the size of the bolus entering the throat and then estimates the percentage of bolus remaining within the throat after the swallow (i.e., valleculae, pharyngeal wall, and pyriform sinuses).
Note: Dr. Catriona Steele’s Swallowing Rehabilitation Research Lab is currently working on better pixel based scalers to better quantify residue and to answer the question of how much residue is too much. More on that soon!
The final combined score is the Overall DIGEST Grade. The 0 to 4 rating scale was chosen to help communicate severity with the oncology team, who already use similar ratings in the Common Terminology Criteria for Adverse Events (CTCAE) scale. This is great for multidisciplinary care! For example, an Overall DIGEST Grade 3 of severe may indicate severe dysphagia with potentially significant alterations of diet and tube feedings to supplement. Grade 3 on the CTCAE may not yet be life-threatening (as in Grade 4), but it does also indicate that the person is experiencing a severe medical impact, may require hospitalization, and may be limited in completing activities of daily living (ADLs).
Let’s update dysphagia clinicians on the expanding the utility of DIGESTv2:
Cross-Cultural Translation
To facilitate international standardized toxicity reporting, Dr. Renata Lígia Vieira Guedes and colleagues (2025) worked with Hutcheson’s team to develop the formal Brazilian Portuguese translation and cultural adaptation of DIGESTv2. This ensures that Brazilian oncology networks can track and compare pharyngeal safety, efficiency and toxicity data utilizing identical global metric parameters. Dr. Vieira Guedes also translated the MD Anderson Dysphagia Inventory (quality of life scale) into Brazilian Portuguese in 2013. More on this MDADI and other translations below in #7.
Cross-Instrumentals Validation
Originally, DIGEST was created to be used with the MBSS/VFSS. However, Dr. Starmer and colleagues (2021) adapted it for use with flexible endoscopic evaluation of swallowing or FEES. This is called DIGEST-FEES. Then Dr. Curtis and team (2025) demonstrated how VASES (the Visual Analysis of Swallowing Efficiency and Safety) can be used to increase the “transparency and standardization of DIGEST-FEES ratings,” as stated in their abstract.
Cross-Population Validation
While initially created for people with head and neck cancer, the underlying logic of the DIGEST algorithm may be useful in other clinical populations. See issues that arose in an early validation study in the post-stroke population by Dr. Krekeler and team (2026), who compared DIGESTv2 to the MBSImP
Cross-Tools: Mapping DIGEST to IDDSI Framework
In a major step forward for clinical standardization using instrumental evaluations (MBSS or FEES), Hutcheson, Steele, Lam, and Barbon (2025) published a mapping of the IDDSI Framework – with its specific labels of foods and drinks/liquids – onto the DIGEST decision tree. The original DIGEST and DIGESTv2 only refer to “liquids,” “pudding,” and “cracker or cookie,” without specifically using the IDDSI Levels of 0 to 7 or the standardized labels (e.g., Pureed, Level 4). In Dr. Hutcheson, Steele, Lam & Barbon’s Open Access article, you can see Figure 1 that shows provides this mapping to IDDSI standardized terminology.
This use of IDDSI’s standardized labeling will really help remove any ambiguity in the rating process for the Safety Grade and Efficiency Grade. For more on IDDSI, I have written many blogs since 2014, and here is one on IDDSI updates. See also my chapter in this cookbook that thoroughly helps the public consumer understand IDDSI. See IDDSI Framework image discussed in #5 below.
4. High-Intensity Exercise
The Swallowing Boot-Camp: High-Volume Reconditioning
For the last 2 decades, dysphagia therapy has started to focus on neuroplasticity, such as use it or lose it and making sure we do targeted and salient therapy with enough repetitions to make a difference. For example, Dr. Malandraki and team (2016) created an “Intensive Dysphagia Rehabilitation Approach,” for people with neurogenic dysphagia.
Therapy for people with head and neck cancer has to combat the two threats of radiation fibrosis and disuse atrophy. Therefore, in 2012, the MD Anderson team designed a “Boot Camp Swallowing Therapy Program” (Hutcheson et al., 2015). Malandraki & Hutcheson (2018) provide a good history of this the Intensive Dysphagia Rehabilitation Approach versus the Boot Camp. This 2013 article from National Foundation of Swallowing Disorders (NFOSD) highlighted two of the original creators: Denise Barringer, M.S., CCC-SLP and Katherine A. Hutcheson, PhD, Assistant Professor in the Department of Head and Neck Surgery, from the University of Texas MD Anderson Cancer Center. This NFOSD article described this aggressive and high-intensity therapeutic protocol:
“A way to jump start the swallowing process for patients who were having swallowing difficulties after their treatment or had plateaued (some after years) in their efforts to regain their swallowing function. Boot camp swallowing therapy is an aggressive program of swallowing treatment tailored to the individual and is generally conducted over a three week period.”
This evidence-based program moves away from passive, low-load home exercise packets. I wanted to focus on the idea of BOOT CAMP as a separate update in this blog, as that really drives home the idea that people need to prepare to fight through the sometimes horrible challenges of chemoradiation treatment. As I noted in this article, when actor Michael Douglas had oropharyngeal head and neck cancer, he equated treatment to a well-planned war. Michael Douglas had HPV+ cancer and was misdiagnosed 3 times before he was able to start his fight.
Phase 1: The Optimization Phase
Prior to entering the high-intensity swallowing therapy, people require comprehensive evaluations to identify and manage barriers to swallowing, such as (not a complete list):
- Esophageal strictures: esophageal dilation to clear physical obstructions or narrowings.
- Device-driven respiratory training (see EMST section below) to maximize physiological reserves and ability to cough and eject aspiration.
- Testing with and optimizing lingual strength with objective resistance devices such as the IOPI (Iowa Oral Performance Instrument).
Phase 2: The Intensive Exercise Phase
This is a short but intense 2 to 3-week program. It is described by Hutcheson and team (2015) as “mass practice” and “progressive resistance model.” This idea is described further below in the formalized PRO-ACTIVE therapy model. Under direct guidance by the SLP, this boot camp uses progressive overload with eating plus exercising.
Historical Note: In 2010, the McNeill Dysphagia Therapy Program proposed a new model of using intentional and challenging swallowing trials, thinking of food as “weights.” The weight lifting or strength training happens with effortful swallows of progressively more challenging foods, from a smoothie that may be mildly thick to a pureed food to soft & bite-sized foods to easy to chew and finally regular textures (per IDDSI Framework).
More on this Eat + Exercise concept below in this next section on use it or lose it.
5. Use it or Lose it: PRO-ACTIVE Therapy & EAT-RT Staircase
The Danger of Complete Feeding Tube Dependency
When a person is in the middle to end of radiation therapy, the pain and acute radiation mucositis can be so excruciating that the person may be tempted to not eat anything at all. The doctor may even order a strict NPO status (nothing by mouth). In the past, a Percutaneous Endoscopic Gastrostomy tube (PEG feeding tube) was often placed before treatment started for all hydration and nutrition needs.
However, research has demonstrated that shutting down the swallowing system during cancer treatment triggers a dangerous secondary pathology. A landmark study by Langmore et al. (2012) evaluated whether prolonged PEG use actively worsened long-term swallowing outcomes. Their findings revealed that total oral restriction resulted in more severe disuse atrophy (wasting/weakening) of the pharyngeal and laryngeal musculature. Those research participants who were at least able to eat something – even if the PEG was used for supplemental feedings and hydration – had better swallows in the long run.
As much as you can, you want to load the muscles through eating and drinking. The combination of disuse atrophy and progressive tissue fibrosis or stiffness can really reduce the swallowing safety and efficiency, as well as causing issues such as long-term narrowing or esophageal strictures.
How else can we help reduce the radiation-associated dysphagia?
Proactive vs. Reactive Intervention for Head and Neck Cancer: Evidence from the PRO-ACTIVE Trial
For many years, the standard of care for managing dysphagia in head and neck cancer was entirely reactive (i.e., well after the dysphagia started). Speech-Language Pathologists (SLPs) were typically consulted months after cancer treatments ended. Sometimes SLP consult orders were finally received during the person’s hospitalization due to a severe aspiration pneumonia or a stricture (narrowing of the pharyngoesophageal segment – at the top of the esophagus).
This passive-reactive therapy has been flipped to proactive by landmark clinical protocols from the PRO-ACTIVE Trial (Hutcheson et al., 2020; Martino, … & Hutcheson et al., 2021; Hutcheson et al., 2025). This was an international, multi-site effort that included almost 1,000 people who were deemed high risk for post-radiation dysphagia (RAD). The PRO-ACTIVE intervention group (1 out of 3 arms of this randomized control trial) included “EAT + EXERCISE” with high intensity therapy BEFORE radiation started (Hutcheson et al., 2020; Martino et al., 2021).
One of the core principles that helped create PRO-ACTIVE therapy was the concept of Eat-All Through Radiation Therapy (or EAT-RT), which was developed by Princess Margaret Cancer Centre in Canada (Dr. Martino) and MD Anderson Cancer Center in Texas (Dr. Hutcheson) and colleagues with this 2020 publication.
To see one key part of this program, check out the EAT-RT STAIRCASE in this link — Find Figure A1 in Appendix C.
This EAT-RT staircase may guide the person down the staircase to foods like high calorie smoothies (from this blog) during the worst of the acute radiation toxicities. However, the staircase also guides the person back up to work the muscles with more and more solid foods to maintain oral intake through chemoradiation and beyond. Every day may be different, but if you understand the staircase idea, you can make the necessary modifications and take your days one step at a time.
People with dysphagia from head and neck cancer may take each day one step at a time. Additionally, the SLP (dysphagia clinician) can help you step down to foods and drinks that may be easier and safer to swallow OR step up the challenge of foods and liquids again as you recover after your chemoradiation treatments and beyond.
Proactive pre-habilitation of pushing eating as exercise and performing swallowing exercises before and even during radiation – to the best of your ability – can help reduce the later effects of radiation fibrosis. It can reduce disuse atrophy. This works the muscles of the tongue, jaw, and pharynx through strengthening and range of motion exercises prior to the onset of tissue scarring.
The clinician also helps educate and counsel the person to personalize oral intake, manage pain, and help address the struggles with the rest of the medical team. People are coached to maintain a safe oral diet throughout the entire trajectory of their radiation treatment. To safely facilitate these diet changes, clinicians teach and monitor eating along the EAT-RT staircase. Note: See the IDDSI food and drinks/liquids pyramids below with IDDSI Levels from Thin liquid, Level 0 to Regular diet, Level 7. IDDSI easily matches the staircase idea. You may eat up or down through the Levels 0 to 7.
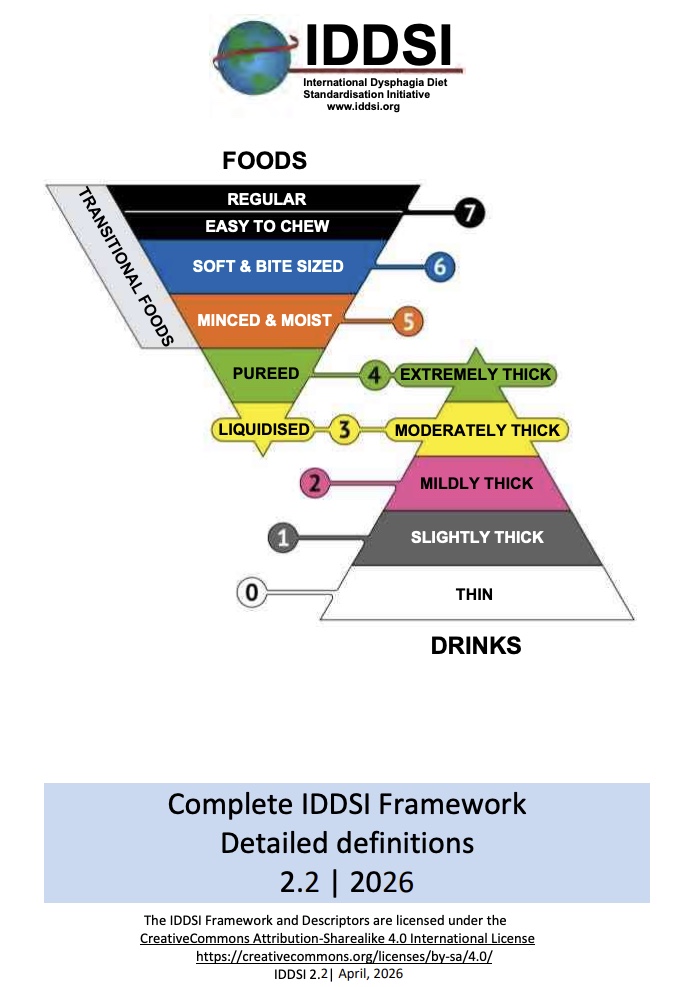
IDDSI Framework is a living document. See this 2.2 2026 Version with links to the Framework and Testing Methods in many languages here.
When the person is ready to work back up the staircase, or back up the IDDSI Levels, food as “weight” is paired with swallow strategies such as the effortful swallow (swallow hard, pushing with your tongue and squeezing with your throat muscles).
PRO-ACTIVE therapy neuroplastic principle: “Use It or Lose It.”
Rationale: Maximizing pharyngeal activity during RT through exercise and eating may improve outcomes in all patients
Goals:
- Perform pharyngeal swallow exercise during RT;
- Keep eating most challenging foods possible during RT (individualized plan);
- Swallow strong (effortful swallow) if necessary to help clear food.
6. Fortify the System: Cough Strength
For people with acute to chronic radiation-associated dysphagia, there may be significant safety issues. They may have difficulty protecting their airway during a swallow of thin liquids, or they may have food and liquid falling into the airway after the swallow due to the residue in the throat. This requires looking beyond exercises meant to reduce the underlying issues. Sometimes we have to improve the person’s protective defensive mechanisms.
In other words, for many people, we know that liquids, saliva, and food particles are getting down the wrong way (i.e., penetration into voice box and aspiration of dropping below the vocal cords into the trachea). Therefore, we have to improve the person’s ability to cough and expel this material out of the airway.
Expiratory Muscle Strength Training (EMST)
Many people with chronic dysphagia (late-RAD) have reduced sensation and may have frequent aspiration that does not trigger an explosive cough response at all (silent aspiration). Dr. Hutcheson and team (2018) wondered if specifically working on Expiratory Muscle Strength Training (EMST) would improve the cough to eject aspiration and reduce the negative outcomes of dysphagia and aspiration.
By training people to exhale forcefully against a calibrated, spring-loaded mechanical valve, the EMST systematically overloads and strengthens the expiratory abdominal and intercostal muscles. This targeted, device-driven therapy significantly improved the maximum expiratory pressure generation (MEP), which was reduced in people with RAD. The 2018 study also showed improvements on the safety scores of the DIGEST and quality of life scores. Manduchi and team (2026) also showed progress in safety and upgrades to their IDDSI levels on this food and liquid framework.
7. Holistic Care for Dysphagia from Head and Neck Cancer
Person-Centered Outcome Scales
A comprehensive dysphagia evaluation with fluoroscopy and/or endoscopy coupled with targeted dysphagia therapy is only half the picture. We must also capture the personal, emotional, and social impacts of living with a chronic swallowing disorder. These quality of life tracking scales are called Person-Reported Outcome Measures (PROM). You may have seen the more general 10-question scale – the Eating Assessment Tool or EAT-10 (which has been highly researched and translated into many languages).
For tracking quality of life in people with head and neck cancer, use the more thorough M.D. Anderson Dysphagia Inventory (MDADI).
The MDADI is a validated, self-administered psychometric questionnaire that measures the specific physical, emotional, and functional impacts of swallowing difficulties from the person’s perspective. Whether evaluating a young HPV-positive survivor navigating acute toxicities or another person managing the 6 months to 2-year progressive fibrotic and neurological changes, the MDADI ensures that the clinical team’s focus is on the individual’s needs. Treatment targets align with the person’s actual lived experience and individual goals of care. (Links in prior sentence are to further research on the MDADI in HPV-positive and in those up to 2-year post onset.)
MDADI Translations:
Dutch version expanded for neurological disease
Swedish (expanded use for people with neurological disease too)
Turkish (expanded use to people with neurological disease too)
More Resources for Holistic Head and Neck Cancer Care
1. Continuing Education at AB-SSD
See the American Board of Swallowing and Swallowing Disorders (AB-SSD) Continuing Education courses page:
“Holistic Dysphagia Management for People with Head and Neck Cancer”
Course Description: “This is a joint presentation by an Otolaryngologist, Tanya K. Meyer, MD, and a Speech Pathologist, Jan Carol Pryor PhD, CCC-SLP, BCS-S, on the topic of Holistic Management of People with Dysphagia due to Head and Neck Cancer (HNC).
Many people diagnosed with HNC experience challenging obstacles during cancer treatment, shortly after surgery +/- radiation, and many years later. Historically, the medical rehabilitation model has focused on physical impairment. However, qualitative research with people with HNC has identified that dysphagia impacts more than physical function, compromising psychological and social health. Therefore, the aim of the presentation is to provide ideas for a personalized approach to dysphagia management from an interdisciplinary perspective with the goal of positively impacting quality of life. A case study format will be used to elucidate challenging scenarios and personalized interventions.”
Here is the link again: https://www.swallowingdisorders.org/page/HolisticDysphagiaManagement
2. Dysphagia Support at NFOSD
The National Foundation of Swallowing Disorders (NFOSD):
![]()
Find your local support group here: https://swallowingdisorderfoundation.com/nfosd-support-groups/
At the link above, NFOSD shares what their Members of dysphagia support groups report:
- Feeling less lonely, isolated, anxious, depressed, or judged
- Gaining a sense of empowerment and control
- Being able to talk openly and honestly about one’s feelings
- Getting practical advice or information about treatment and coping options
- Comparing notes about resources, such as doctors and alternative options
3. Dysphagia Education at NFOSD
Check out NFOSD’s library of webinars here. Here are some highlighted topics for head and neck cancer:
- Survivorship: Carie Montesa, MSN, RN, AGACNP-BC & Liza Blumenfeld, MS, CCC-SLP, BCS-S shared: “Survivorship 101: Navigating Head and Neck Cancer at Diagnosis, Treatment and Beyond.”
- Oral Health: Karen Sheffler from SwallowStudy.com shared: “More than Oral Care – Let’s Talk Oral Infection Control.” This webinar focused on the importance of oral hygiene to help reduce the risks of aspiration pneumonia. Please see more of my articles on oral infection control here, as keeping the mouth clean, moist, and comfortable is a key to treatment in head and neck cancer:
- Self-Screening: Jo-Anne Jones, RDH, FIADFE (Dentist) shared: “Screening and Self-Exam Essentials for Head and Neck Cancer: What YOU Need to Know”
- HPV: Ezra Cohen, MD, FRCPSC, FASCO (Oncologist) shared: “Modern Day Head and Neck Cancer.” This reported that HPV+ head and neck cancers are on the rise, but they have better prognosis and treatments have been de-intensified to improve swallowing function long-term.
Clinical Summary Matrix for Head and Neck Cancer
| Evaluation or Therapy Area | Primary Goals | Evidence & Tools |
| Standardization of Dysphagia Severity Ratings | Provide objective, reproducible tracking of pharyngeal swallow safety and efficiency across global clinical networks. Allows the dysphagia specialist to use the same rating scales/terminology as the oncologist. Tracks decline to progress over time. | DIGESTv2 (Version 2) |
| Testing Protocol Standardization to IDDSI | Eliminate ambiguity by using the IDDSI Framework with its clear labels of each food and drink LEVEL.
This provides a global standard to the DIGEST protocol, as IDDSI provides a global framework to describe, label, and test consistency and viscosity (thickness) all foods and drinks. |
DIGEST-to-IDDSI Decision Tree Mapping |
| PRO-ACTIVE Pre-Rehabilitation | Reduce disuse atrophy & progressive tissue fibrosis.
Preserve oral and pharyngeal strength and range of motion with early, high-load eating and exercise. Start before radiation. |
PRO-ACTIVE Therapy Manuals |
| Intense Therapy & Maintenance of Oral Diet | Counteract fibrosis and acute/chronic disuse muscular atrophy and minimize long-term feeding tube dependency. | PEG Avoidance Analysis (Langmore et al., 2012)
MD Anderson Swallowing Boot-Camp Protocols & Intensive Dysphagia Rehabilitation (Review: Malandraki, G.A. & Hutcheson, K.A., 2018) |
| Airway Defensive Mechanisms | Increase maximum expiratory pressure to maximize volitional and reflexive cough, reducing aspiration pneumonia. | Expiratory Muscle Strength Training / EMST |
| Person-Reported Outcome Measures | Capture and track the multi-dimensional physical, functional, and emotional burden of chronic dysphagia on daily living. | M.D. Anderson Dysphagia Inventory (MDADI) (Chen et al., 2001)
See all links in #7 above |
*******
Thank you as always for reading & sharing — especially during the Dysphagia Awareness Month.
See my other Dysphagia Awareness Month articles here:
Dysphagia Awareness Month: What You Need to Know
Rewiring Neurogenic Dysphagia: Finding Hope in the Brain-Swallow Connection
Deep Dive into Esophageal Dysphagia + 10 Questions
Older one: Why We Need Dysphagia Awareness Month
References for Dysphagia in Head and Neck Cancer
- Abreu, M., Oliveira, D. M. A., Bastos Neto, B. C., Germano, J. N., Kowalski, L. P., & Curado, M. P. (2025). Overall and disease-free survival in patients with HPV-positive and HPV-negative oropharyngeal cancer. Einstein (Sao Paulo, Brazil), 23, eAO1525. https://doi.org/10.31744/einstein_journal/2025AO1525; https://pmc.ncbi.nlm.nih.gov/articles/PMC12539820/
- Carnaby-Mann, G. D., & Crary, M. A. (2010). McNeill dysphagia therapy program: a case-control study. Archives of physical medicine and rehabilitation, 91(5), 743–749. https://doi.org/10.1016/j.apmr.2010.01.013
- Chen, A. Y., Frankowski, R., Bishop-Leone, J., Hebert, T., Leyk, S., Lewin, J., & Goepfert, H. (2001). The development and validation of a dysphagia-specific quality-of-life questionnaire for patients with head and neck cancer: the M. D. Anderson dysphagia inventory [MDADI]. Archives of otolaryngology–head & neck surgery, 127(7), 870–876. https://pubmed.ncbi.nlm.nih.gov/11448365/
- Chen, C., Lohavanichbutr, P., Zhang, Y., Houck, J. R., Upton, M. P., Abedi-Ardekani, B., Agudo, A., Ahrens, W., Alemany, L., Anantharaman, D., Conway, D. I., Futran, N. D., Holcatova, I., Günther, K., Hansen, B. T., Healy, C. M., Itani, D., Kjaerheim, K., Monroe, M. M., Thomson, P. J., … Wang, P. (2020). Prediction of survival of HPV16-negative, p16-negative oral cavity cancer patients using a 13-gene signature: A multicenter study using FFPE samples. Oral oncology, 100, 104487. https://doi.org/10.1016/j.oraloncology.2019.104487
- Curtis, J. A., Tabor Gray, L., Arrese, L., Borders, J. C., & Starmer, H. (2025). Characterizing the Validity of Using VASES to Derive DIGEST-FEES Grades. Folia phoniatrica et logopaedica : official organ of the International Association of Logopedics and Phoniatrics (IALP), 77(1), 10–19. https://doi.org/10.1159/000538935
- Guedes, R. L., Angelis, E. C., Chen, A. Y., Kowalski, L. P., & Vartanian, J. G. (2013). Validation and application of the M.D. Anderson Dysphagia Inventory in patients treated for head and neck cancer in Brazil. Dysphagia, 28(1), 24–32. https://doi.org/10.1007/s00455-012-9409-x
- Hutcheson, K. A., Steele, C. M., Lam, P., & Barbon, C. E. A. (2026). Mapping the DIGEST Decision Tree to the IDDSI Framework to Promote Reproducibility and Global Implementation. Dysphagia, 10.1007/s00455-026-10943-6. Advance online publication. https://doi.org/10.1007/s00455-026-10943-6
- Hutcheson, K. A., Martino, R., PRO-ACTIVE Trial Working Group, PRO-ACTIVE Trial Speech-Language Pathologist Working Group. (2025). Therapy Manuals for Clinically Implementing Proactive and Reactive Swallowing Therapies During Head and Neck Radiotherapy: Using the TIDieR Framework to Disseminate PRO-ACTIVE Trial Interventions. Perspectives of the ASHA Special Interest Groups, 10(6), 2032-4048. https://pubs.asha.org/doi/10.1044/2025_PERSP-25-00093
- Hutcheson, K. A., Barbon, C. E. A., Alvarez, C. P., & Warneke, C. L. (2022). Refining measurement of swallowing safety in the Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) criteria: Validation of DIGEST version 2. Cancer, 128(7), 1458–1466. https://doi.org/10.1002/cncr.34079
- Hutcheson, K. A., Gomes, A., Rodriguez, V., Barringer, D., Khan, M., & Martino, R. (2020). Eat All Through Radiation Therapy (EAT-RT): Structured therapy model to facilitate continued oral intake through head and neck radiotherapy-User acceptance and content validation. Head & neck, 42(9), 2390–2396. https://doi.org/10.1002/hed.26250
- Hutcheson, K. A., Barrow, M. P., Plowman, E. K., Lai, S. Y., Fuller, C. D., Barringer, D. A., Eapen, G., Wang, Y., Hubbard, R., Jimenez, S. K., Little, L. G., & Lewin, J. S. (2018). Expiratory muscle strength training for radiation-associated aspiration after head and neck cancer: A case series. The Laryngoscope, 128(5), 1044–1051. https://doi.org/10.1002/lary.26845
- Hutcheson, K. A., Barrow, M. P., Barringer, D. A., Knott, J. K., Lin, H. Y., Weber, R. S., Fuller, C. D., Lai, S. Y., Alvarez, C. P., Raut, J., Lazarus, C. L., May, A., Patterson, J., Roe, J. W., Starmer, H. M., & Lewin, J. S. (2017). Dynamic Imaging Grade of Swallowing Toxicity (DIGEST): Scale development and validation. Cancer, 123(1), 62–70. https://doi.org/10.1002/cncr.30283
- Hutcheson, K. A., Barrow, M. P., Plowman, E. K., Lai, S. Y., Fuller, C. D., Barringer, D. A., . . . Lewin, J. S. (2017). Expiratory muscle strength training for radiation-associated aspiration after head and neck cancer: A case series. Laryngoscope, 128, 1044–1051. https://doi.org/10.1002/lary.26845
- Hutcheson, K. A., Kelly, S., Barrow, M. P., Barringer, M. S., Perez, D. G., Little, L. G., . . . Lewin, J. S. (2015). Offering more for persistent dysphagia after head and neck cancer: The evolution of boot camp swallowing therapy. Paper presented at the Combined Otolaryngology Spring Meeting, Boston, MA.
- Hutcheson, K. A. (2013a). Late radiation-associated dysphagia (RAD) in head and neck cancer survivors. Perspectives on Swallowing and Swallowing Disorders (Dysphagia), 22(2), 61–72. https://doi.org/10.1044/sasd22.2.61
- Hutcheson, K. A., Bhayani, M. K., Beadle, B. M., Gold, K. A., Shinn, E. H., Lai, S. Y., & Lewin, J. (2013b). Eat and exercise during radiotherapy or chemoradiotherapy for pharyngeal cancers: Use it or lose it. JAMA Otolaryngology—Head & Neck Surgery, 139(11), 1127–1134. https://doi.org/10.1001/jamaoto.2013.4715
- Hutcheson, K. A., Barringer, D. A., Rosenthal, D. I., May, A. H., Roberts, D. B., & Lewin, J. S. (2008). Swallowing outcomes after radiotherapy for laryngeal carcinoma. Arch Otolaryngol Head Neck Surg, 134(2), 178-183. https://doi.org/10.1001/archoto.2007.33
- Krekeler, B. N., Hopkins, A., Vollman, C., Davidson, K., Broderick, E., Altaye, M., Tabangin, M., Martin-Harris, B., & Hutcheson, K. A. (2025). Preliminary Validation of Dynamic Imaging Grade of Swallowing Toxicity (DIGEST(V2)) for Characterizing Swallow Safety and Efficiency in Post-Stroke Populations. Dysphagia, 41(1), 96-104. PMID: 40810807.
- Johnson, J. (2016, February). Oropharyngeal Cancer in the Era of HPV. Session presented at the Post-Graduate Course: Something You Can Chew On: Evidence-based Dysphagia Clinical Care at the Dysphagia Research Society 2016 Annual Meeting, Tucson, AZ.
- Langmore, S., Krisciunas, G. P., Miloro, K. V., Evans, S. R., & Cheng, D. M. (2012). Does PEG use cause dysphagia in head and neck cancer patients?. Dysphagia, 27(2), 251–259. https://doi.org/10.1007/s00455-011-9360-2
- Lin, B. M., Wang, H., D’Souza, G., Zhang, Z., Fakhry, C., Joseph, A. W., … Pai, S. I. (2013). Long term prognosis and risk factors among HPV-associated oropharyngeal squamous cell carcinoma patients. Cancer, 119(19), 3462–3471. https://doi.org/10.1002/cncr.28250
- Loy, R. D., Rogus-Pulia, N., Ketchum, F., Troche, M., Rameau, A., Jones, H. N., Riquelme, L., Gilmore-Bykovskyi, A., Shah, M. N., & Kind, A. (2025). Eating and swallowing care disparities in persons with dementia: A conceptual framework. Alzheimer’s & dementia : the journal of the Alzheimer’s Association, 21(2), e70028. https://doi.org/10.1002/alz.70028
- Manduchi, B., Warneke, C.L., Barrow, M. P. Barrow, et al. (2026). Expiratory Muscle Strength Training in Head and Neck Cancer Survivors With Radiation-Associated Dysphagia: Results of a Pilot Prospective Trial, Head & Neck, 1–12, https://doi.org/10.1002/hed.70273
- Malandraki, G. A., Rajappa, A., Kantarcigil, C., Wagner, E., Ivey, C., & Youse, K. (2016). The Intensive Dysphagia Rehabilitation Approach Applied to Patients With Neurogenic Dysphagia: A Case Series Design Study. Archives of physical medicine and rehabilitation, 97(4), 567–574. https://doi.org/10.1016/j.apmr.2015.11.019
- Malandraki, G.A., & Hutcheson, K.A. (2018). Intensive Therapies for Dysphagia: Implementation of the Intensive Dysphagia Rehabilitation and the MD Anderson Swallowing Boot Camp Approaches. Perspectives of the ASHA Special Interest Groups, 3, 133-145. https://pubs.asha.org/doi/abs/10.1044/persp3.SIG13.133
- Martino, R., Fitch, M. I., Fuller, C. D., Hope, A., Krisciunas, G., Langmore, S. E., Lazarus, C., Macdonald, C. L., McCulloch, T., Mills, G., Palma, D. A., Pytynia, K., Ringash, J., Sultanem, K., Theurer, J., Thorpe, K. E., & Hutcheson, K. (2021). The PRO-ACTIVE trial protocol: a randomized study comparing the effectiveness of PROphylACTic swallow InterVEntion for patients receiving radiotherapy for head and neck cancer. BMC cancer, 21(1), 1100. https://doi.org/10.1186/s12885-021-08826-0
- Radoï, L., Barul, C., Menvielle, G., Carton, M., Matrat, M., Sanchez, M., Pilorget, C., Velten, M., Stücker, I., Luce, D., & ICARE Study Group (2018). Risk factors for salivary gland cancers in France: Results from a case-control study, the ICARE study. Oral oncology, 80, 56–63. https://doi.org/10.1016/j.oraloncology.2018.03.019
- Sun, H., Yu, M., An, Z., Liang, F., Sun, B., Liu, Y., & Zhang, S. (2025). Global burden of head and neck cancer: Epidemiological transitions, inequities, and projections to 2050. Frontiers in oncology, 15, 1665019. https://doi.org/10.3389/fonc.2025.1665019
- Starmer, H. M., Arrese, L., Langmore, S., Ma, Y., Murray, J., Patterson, J., Pisegna, J., Roe, J., Tabor-Gray, L., & Hutcheson, K. (2021). Adaptation and Validation of the Dynamic Imaging Grade of Swallowing Toxicity for Flexible Endoscopic Evaluation of Swallowing: DIGEST-FEES. Journal of speech, language, and hearing research : JSLHR, 64(6), 1802–1810. https://doi.org/10.1044/2021_JSLHR-21-00014
- Vieira Guedes, R. L., Silva de Freitas, A., Arakawa Sugueno, L., Hutcheson, K. A., & Pernambuco, L. (2025). Brazilian Portuguese Translation and Cultural Adaptation of the Dynamic Imaging Grade of Swallowing Toxicity version 2 (DIGESTv2). CoDAS. e-Pub ahead of print.