
COVID-19 and Dysphagia Outcomes
by Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
COVID-19 and Dysphagia Outcomes in one acute care hospital. Findings may have been similar around the world.
Introduction to COVID-19 and Dysphagia Outcomes
This article was written from the July 2021 viewpoint.
It has been well over one year since the start of the COVID-19 pandemic that changed our medical speech-language pathology (SLP) practice patterns and staffing so urgently. Fortunately, there was guidance from many experts around the world to help guide SLPs (aka, speech-language therapists / SLTs in other parts of the world) through the uncertainty and fog. Special thanks goes out to the Dysphagia Research Society’s COVID-19 Task Force.
Now, we will start to see more research publications based on months of gathering and analyzing data regarding COVID-19 and dysphagia outcomes in people who required prolonged hospitalizations. Here are some examples of questions that we may be asking regarding dysphagia:
- How many people needed to be intubated? Trached? And for how long?
- How many people suffered from post-extubation dysphagia and other sequela?
- How many people required an SLP evaluation?
- How many needed to be held NPO?
- Did the long lengths of intubation correlate with how long people took to restart oral intake?
- Were people started on modified diets and thickened liquids more often than regular diets?
- Were people with dysphagia readmitted with aspiration pneumonias or other prolonged negative sequela?
Dysphagia: Under-Identified Iatrogenic Problem
During #DysphagiaAwareness month (June), we need to raise awareness of this often silent difficulty swallowing (dysphagia). Dysphagia is a symptom of underlying diseases, disorders, or structural abnormalities. However, it is often under-identified. Dysphagia can even be caused by the medical treatments themselves (e.g., medications, intubations, surgeries and other medical procedures). This last point describes the term: Iatrogenic.
Iatrogenic symptoms or conditions are those that are caused by the medical treatments required to cure or treat the underlying illness.
For example, people fighting COVID-19 required prolonged intubations, and that treatment caused post-extubation dysphagia, which is the iatrogenic condition.
People also required tracheostomies if they could not be extubated.
Still others required high-flow oxygen via specialized oxygen delivery systems.
As you see in my prior blogs linked above, all of these medical treatments can cause their own unique dysphagia risks. If the dysphagia is not identified quickly, it could lead to hospital-acquired infections, re-intubations, and even death. To reiterate, too often dysphagia goes under-identified, under-referred, under-evaluated, and under-treated, which not only costs lives and affects the quality of lives, but it also costs billions of healthcare dollars, per Patel & team (2018).
Patel and colleagues urged in their article’s implications section:
“It behooves clinicians and hospitals to recognize and treat dysphagia early to reduce the risk of in-hospital mortality.”
So, now we ask:
How did providers do during COVID-19 surge and beyond?
Dr. Camilla Dawson, DClinP, BSc(hons) MRCSLT, MHCPC, an SLP/SLT from the Queen Elizabeth Hospital in Birmingham, UK, started answering our COVID-19 pandemic and dysphagia management questions — along with her huge team of authors/researchers (See Dawson, et al., 2020, in The Journal of Laryngology & Otology; Link: https://pubmed.ncbi.nlm.nih.gov/33168109/). Their article titled: “Dysphagia Presentation and Management Following Coronavirus disease 2019: An Acute Care Tertiary Centre Experience,” was first published online in November 2020.
Dawson shared:
“Unfortunately our hospital Trust saw over 13,000 patients from March 2020 to March 2021, the most patients in a single centre in the UK. Whilst a sobering number, this has allowed us to analyse our data and practice to hopefully help other teams reflect and plan interventions as the pandemic pressures develop across the globe,” (personal Twitter communication on May 26, 2021).
During the surge from March to May 2020, these researchers analyzed the 720 people who were admitted for more than 3 days (out of an approximate total of 1700 total admissions).
Please see some of their interesting data listed and discussed below:
COVID-19 and Dysphagia Outcomes Data from One Hospital
About 42% of people (N=720 out of the approximately 1700 total people admitted to this hospital from March to May 2020) required admission greater than 3 days.
Those 720 people were who this team of researchers analyzed.
- 29% (208 out of 720 people) were referred for SLP evaluations and received targeted therapy as appropriate.
- Referrals were from staff and were based on overt clinical signs, such as: coughing, pain, difficulty swallowing, reduced oral intake, and presumed aspiration events with chest x-ray results.
- Certainly, there may have been dysphagia that was un-recognized and under-referred.
- 28.3% (204 out of 720) required ICU admission for endotracheal intubation and ventilator needs.
- 50% (102 of 204)of those in the ICU required SLP evaluation.
- 80% of those in the ICU who were referred to SLP (82 out of 102) required tracheostomies.
- Based on the initial assessments of those who were actually evaluated in the ICU (only 58 of the 102):
- 33% (19 of 58) were started on a modified diet or liquid (with only one person on an IDDSI Level 7 Easy to Chew diet), while
- 67% (39 of 58) had recommendations to remain NPO.
Infographic on the COVID-19 and Dysphagia Outcomes
(Infographic made by Karen Sheffler for the American Board of Swallowing & Swallowing Disorders/AB-SSD newsletter and social media @BCSSwallowing and @SwallowStudySLP):
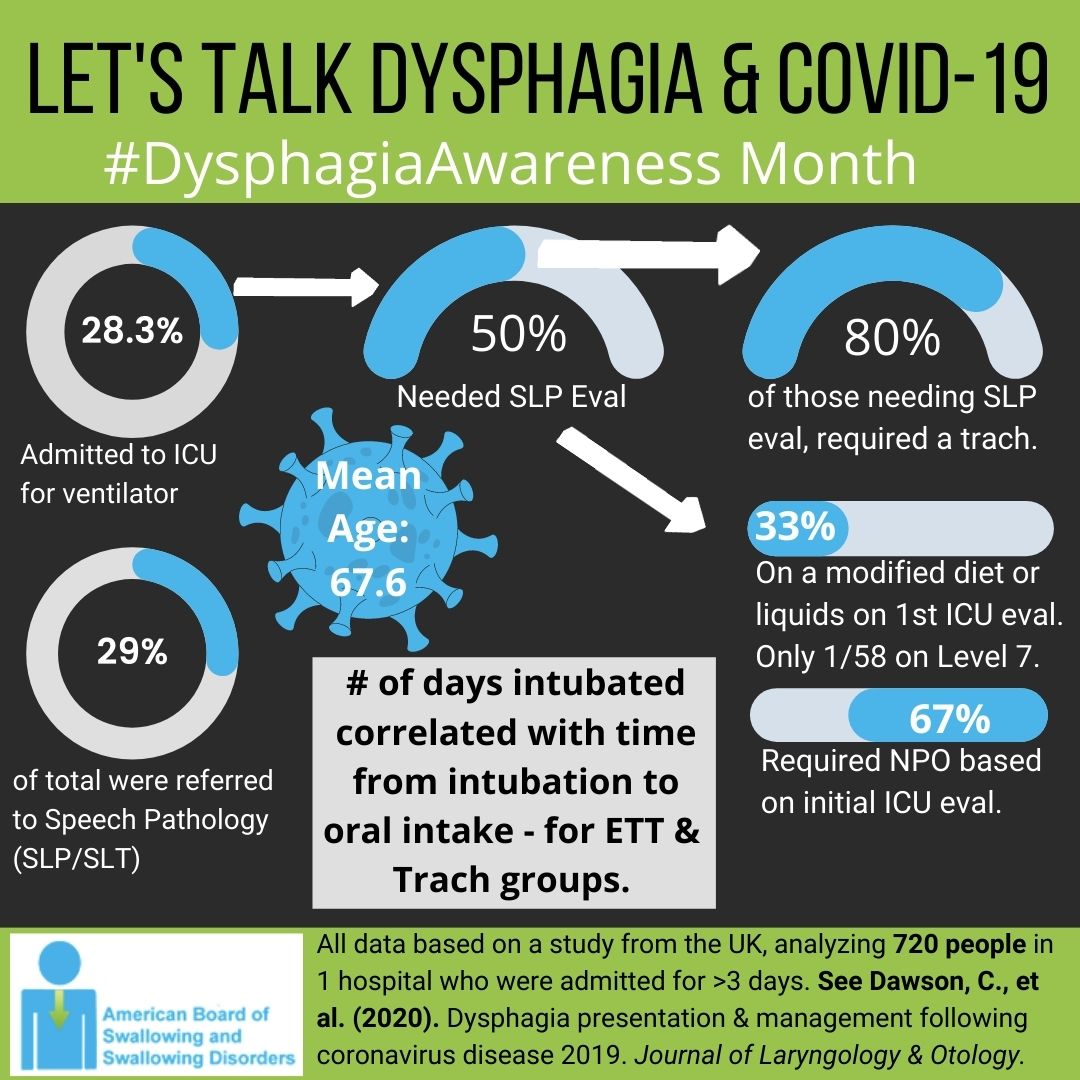
COVD-19 and dysphagia outcomes in this infographic are based on data from this UK study analyzing 720 patients at 1 hospital.
Now let’s look at how people who were on the regular hospital floors did (i.e., on the wards).
- 51% of the total SLP evaluations were for people on the wards (non-ICU).
- 29% (31 out of 106) were started immediately on a Regular diet/IDDSI Level 7. By discharge, the majority of these people on the wards were advanced to an IDDSI Level 6 or 7 diet.
- 22% (23 out of 106) had recommendations for NPO.
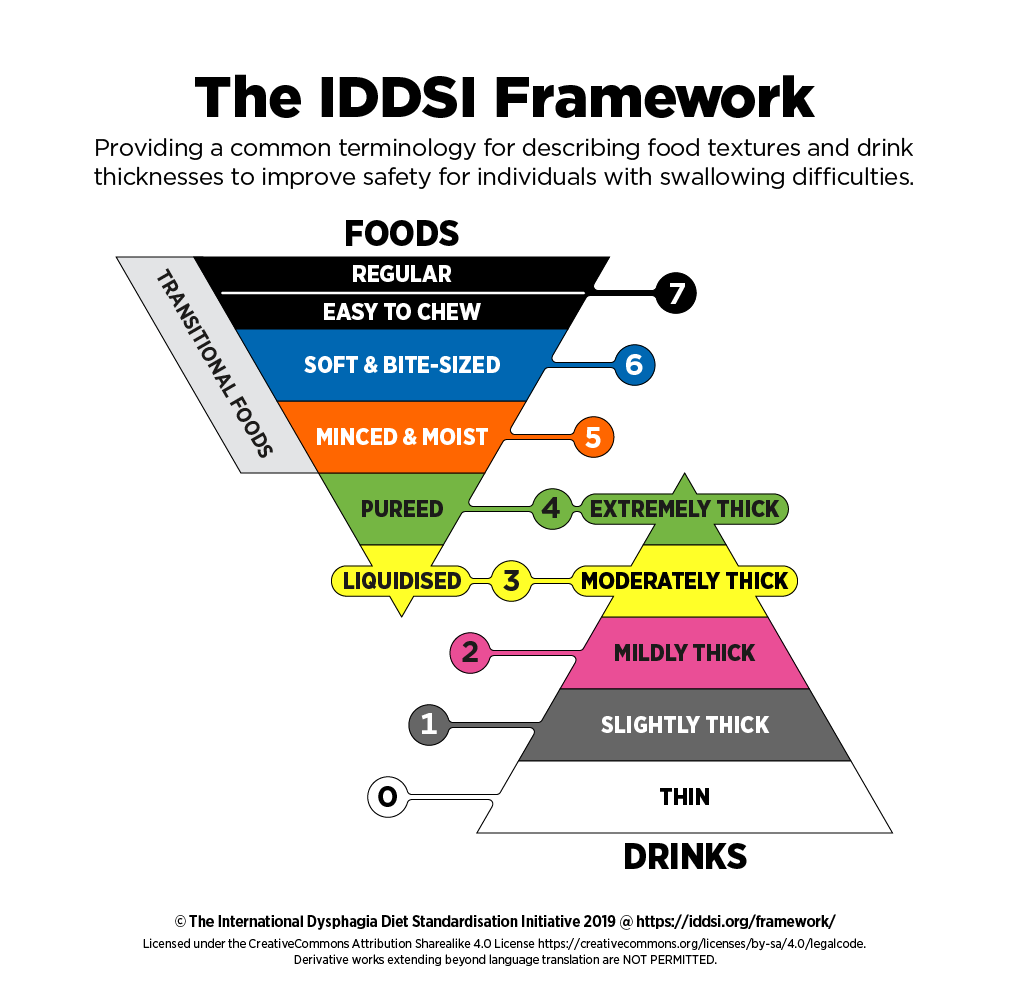
Here is the IDDSI Framework for reference (www.iddsi.org). Isn’t it refreshing how new research can now use an internationally-standardized dysphagia diet. We are finally globally speaking the same language in the clinic and in the research lab. That is a true gift for this June Dysphagia Awareness Month!
- 93% (193 people out of the initial 208 people who were referred to SLP) survived to resume oral intake.
- 20% were taking thickened liquids (39/193). The researchers stated: “thickener is not frequently used in our institution, with postural advice and exercise therapy being preferred,” (page 984).
- 75% were eating a modified diet (145/193).
- 87% of those with tracheostomies required a modified diet versus 59% who were extubated and did not require a tracheostomy.
- People with trachs required more therapy time, including cuff deflation, downsizing trach tubes, and the use of speaking valves to support sensation, cough, and expectoration. Researchers recommended: Support through saline nebulizers kept secretions thinned and able to be mobilized, and this worked better than secretion-drying agents.
- 18% of those who were intubated/extubated were recommended for thickened liquids, versus only 4% of the people with tracheostomies. As opposed to the higher number of people on the wards on thickened liquids (36%). In addition to their tendency to not use thickened liquids, I also wonder if this was due to less close monitoring on the wards versus the ICUs, and therefore, the SLPs had more conservative recommendations. It may have been also due to the use of more definitive testing (e.g., fiberoptic endoscopic evaluation of swallowing / FEES) on some more complex ICU patients.
- How quickly were people able to start oral intake?
- Mean time from extubation to starting oral intake: 5.3 days (SD = 2.3 days).
- Mean time from tracheostomy placement to oral intake: 14.8 days (SD = 6.6 days).
- Mean time for the tracheostomy group from cessation of sedation to oral intake: 13.0 days (SD = 6.0 days).
- Mean time from intubation, through tracheostomy, to oral intake: 28.0 days (SD = 8.5 days).
- Mean time from intubation to extubation to oral intake: 15.8 days (SD = 6.2 days).
- Statistically significant positive correlation only seen in the following groups regarding when oral intake was started:
- For the endotracheal tube (ETT) group: Number of days from intubation to the start of oral intake.
- For the tracheostomy group: Number of days from intubation to the start of oral intake.
- This shows that it was the amount of time intubated that was the most significant factor in delay to oral intake, rather than sedation or time post-extubation, or even time post-tracheostomy insertion. That is consistent with anecdotal reports during COVID-19 of extremely long intubations and the potential for post-extubation dysphagia.
- How much therapy did they require on average?
- 6 days for those who were not intubated or trached.
- People in the ICU required significantly more days than people in the ward.
- 3 days for those who had ETT.
- 9 days for those with trachs.
- These numbers did not include the extensive indirect therapy time, consulting with and communicating with the multidisciplinary team.
Dysphagia Was Complicated by Many Factors
It is important to highlight and document concomitant factors that are noted during our comprehensive clinical/bedside swallowing evaluations. Researchers noted: “dysphagia was complicated by:
- Delirium [hyperactive or hypoactive],
- Use of sedation,
- Frequent expectoration of high-volume secretions, and
- Significant fatigue.” (page 983)
They also questioned the effects of:
- Proning,
- Trauma of prolonged critical illness and critical care,
- Reduced translation/interpreter services within infectious areas, causing a significant communication barrier to people for whom English was not their first language,
- Inability to see family members/friends,
- Providing care with PPE, and
- Restrictions placed on aerosol-generating procedures.
Barriers to Oral Intake
The researchers also noted the following barriers to oral intake:
- Neurological compromise
- Respiratory – swallow coordination
- Post-extubation issues
- Vocal cord palsy
- Laryngeal edema
- Pain
- Pervasive laryngeal issues / pervasive voice changes (when these were in conjunction with persistent dysphagia without perceived improvement, the clinicians used fiberoptic endoscopic evaluations of swallowing (FEES) – thereby reducing the use of FEES to only these complex cases).
Per these researchers and clinicians, it was often the “holistic symptom burden” that contributed to recommendations for NPO more so than the suspected overt signs/symptoms of dysphagia and aspiration (page 983).
Dysphagia was Multifactorial & Variable
The dysphagia was multifactorial, per this research, which is typical in critical care. It is so important for SLPs to:
- look at the big picture,
- communicate with the whole team (which has the person and their goals and wishes as the driver of the team), and
- document how these complicating factors/barriers provide the rationale behind the team’s clinical decision-making and recommendations for oral intake options.
Per Dr. Luis Riquelme, PhD, CCC-SLP, BCS-S, from New York City, people with COVID-19 were “fluctuating hour to hour and day to day.” He emphasized that there was significant variability within one person in their ability to breath, stay alert, and take oral intake from one minute to the next and one day to the next. (Please see Dr. Riquelme’s session on how COVID-19 affected our clinical/bedside swallowing evaluation in the ABSSD’s Meet The Masters 2020 Program Titled: COVID, It’s Hard to Swallow: Managing Patients with Dysphagia during the Pandemic).
Unifying Patterns
Despite this multifactorial nature and significant variability within the individual, some patterns did emerge, per Dawson and colleagues (2020):
- Oral dysphagia was commonly seen, causing most people to need a modified diet.
- Some people required thickened liquids for their more overt issues of delirium, fatigue and poor lip closure.
- They were using Slightly Thick / IDDSI Level 1 more often than other thicker levels and found it to be effective for a small number of individuals at the start of their oral intake (page 984).
- Many countries have been using the 5 IDDSI liquid levels for years (e.g., Australia), even with adults. SLPs in America are beginning to adopt the IDDSI framework (see IDDSI Resources blog), because the National Dysphagia Diet (NDD) – or whatever your facility has pieced together – is now obsolete in Diet Manuals as of Fall 2021. Therefore, we could embrace the Slightly Thick level as well. This is the viscosity between thin liquid and mildly thick (old term nectar thick). Maybe you have been jumping to the thicker/less palatable Mildly Thick for years when the person you were evaluating could have benefited from thinner Slightly Thick drinks. If you do not test Slightly Thick in your instrumental examinations, then how do you know?
- Please see article and free CEU opportunity: https://cdn.agilitycms.com/applied-radiology/PDFs/Issues/Bracco_05-21_IDDSI_CE.pdf, where the authors mentioned:
- Slightly Thick can be tested in the videofluoroscopic swallow study/modified barium swallow study using this recipe: 1 part Varibar Nectar thick barium + 1 part Varibar Thin liquid barium – in equal parts and mixed well.
Invest in Staff for Skilled Therapy in Acute Care
Another unifying issue was that people with COVID-19 required a significant investment of staff time to provide appropriate skilled therapy. One can imagine how much time was invested in the indirect support that our service provided to these individuals and staff around cognition, communication and eating/swallowing, as well as caring for the person’s caregivers. Hopefully this insight will provide rehabilitation and speech pathology departments some support for the advocacy needed to maintain adequate staffing!
This attention to therapy was proven successful in Dawson and team’s research cohort, as no one was readmitted with a new aspiration pneumonia after they were discharged to the next level of care. They noted that intensive and “targeted and sustained swallow therapy” was what helped people “regain near normal swallow function prior to discharge” (page 984). The therapy techniques listed in the article were at the level of our professional standard of practice (not extraordinary or novel), as seen on page 982, but a facility does require enough staff to carry out treatments and not just evaluations. Additionally, the SLP department had to use a “whole systems approach,” (page 985) incorporating “medical, surgical, nursing, therapy, and education teams.” They used a person-centered care approach, although the publication did not label it as such, as their targeted treatment reflected that and had good outcomes.
COVID-19 and Dysphagia Outcomes Summary
Dr. Camilla Dawson concluded:
“For me the most important finding was prevalence of dysphagia for approximately 30% of people admitted to our hospital for over 3 days with COVID.
Appropriate funding, infrastructure and recognition of the fundamental role of SLP/SLT in acute services is a core message in our data, and is highlighted by the clinical presentations we describe.
Collaboration of clinical teams created strength and developed our clinical acumen during this complex time, the importance of working together and supporting one another can’t be overlooked.”
(personal communication May 26, 2021).
Hopefully, this research will encourage others to analyze their outcomes. I look forward to hearing from clinicians and researchers. Please share your experiences and other research articles that address similar COVID-19 and dysphagia outcomes (evaluation, management and outcomes data).
Let’s use the motivation of June being #DysphagiaAwareness month to ask tough questions and advocate for our field of speech-language pathology/speech-language therapy. One tough question for clinicians in the United States is that with our staffing cut-backs and cost-saving measures in healthcare, could we have provided this level of targeted treatment (up to 9 days) seen in this UK study?
We strive to provide a prudent and reasonable service within our standard of care for people with difficulty swallowing. Even that level of a practice standard takes a lot of staff time. Clinicians strive to provide excellent-person-centered care, and we often lack the funding and staffing to make that a reality. However, as shown by Patel and colleagues (2018) the social and economic burdens to this country of not appropriately evaluating and treating people with dysphagia are too great to not advocate for more.
*******
Thank you for reading, caring, and sharing!
Here is the Dysphagia Research Society’s COVID-19 Task Force link again:
https://www.dysphagiaresearch.org/page/COVID-19Resources
References
Dawson, C., Capewell, R., Ellis, S., Matthews, S., Adamson, S., Wood, M., Fitch, L., Reid, K., Shaw, M., Wheeler, J., Pracy, P., Nankivell, P., & Sharma, N. (2020). Dysphagia presentation and management following COVID-19: an acute care tertiary centre experience. The Journal of laryngology and otology, 1–6. Advance online publication. https://doi.org/10.1017/S0022215120002443
Patel, D. A., Krishnaswami, S., Steger, E., Conover, E., Vaezi, M. F., Ciucci, M. R., & Francis, D. O. (2018). Economic and survival burden of dysphagia among inpatients in the United States. Diseases of the esophagus : official journal of the International Society for Diseases of the Esophagus, 31(1), 1–7. https://doi.org/10.1093/dote/dox131