
Speaking Valve Springs Hope for Person with COVID-19
by Jessica Lasky, MS, CCC-SLP of Mobile Scope
Additional Tracheostomy/Speaking Valve Resources by Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
In early March of 2020, I didn’t realize how much my life both professionally and personally would change and to what extent. I didn’t realize that I would be on the front lines of an epic battle with an invisible enemy. I certainly never thought I would be in a place of helping lead the charge for speech-language pathologists (SLPs) to provide treatment to a new type of patient. This patient was a person first, who was diagnosed with COVID-19, who had a tracheostomy (aka, trach or trache in British English) placed, and who LIVED to tell the story. This patient, a human being, had been cut off from their family, their friends, and any real human contact for well over a month! When we think in terms of person-centered care, we remind ourselves that these patients are people experiencing intense emotions and surviving in a life that has been turned upside down.
Before all of this, I was a “regular SLP.” I was most concerned about getting every person with difficulty swallowing (dysphagia) safely off of thickened liquids if at all humanly possible with my mobile FEES business. I was lined up to go to a ton of great CEU events throughout this year, and I was thriving.
Then COVID-19 happened.
I was consulted by my critical care team on a person who survived something that was thought to be un-survivable (Read more about this person from AZfamily.com: “Phoenix man one of the first in the world to survive COVID-19 after rare ECMO treatment.”) Then, I was asked to do something no one on the planet had done before. There was NO evidence to guide me, other than the conversations I had with the Intensivists at my hospital.
This person was COVID-19 positive and was intubated for a week (please see prior blog about prolonged intubation and post-extubation dysphagia risks). His medical status was not improving. So, our Pulmonary Intensivists took the leap of faith and performed a tracheostomy on him and placed him on ECMO as a last resort. His organs were shutting down, and his respiratory status was worsening. Amazingly, after several days he was able to be liberated from both ECMO and his ventilator.
First, let me explain what ECMO is very briefly. ECMO is short for Extracorporeal Membrane Oxygenation. It is essentially a heart AND lung bypass, and it is potentially an amazing and lifesaving machine. It is advanced life support, as it removes blood from the body, oxygenates it, and clears the carbon dioxide from the blood. It gives the lungs and heart a rest. It is revolutionary and had, up until several years ago, been primarily utilized in pediatric care or when people were waiting for a lung or heart transplant. We have had ECMO available at my hospital for over a year now, but it is still a new procedure, and its use remains relatively low.
So, once he was off ECMO and off the ventilator, he was breathing on his own through his trach (see picture below to understand the anatomy).
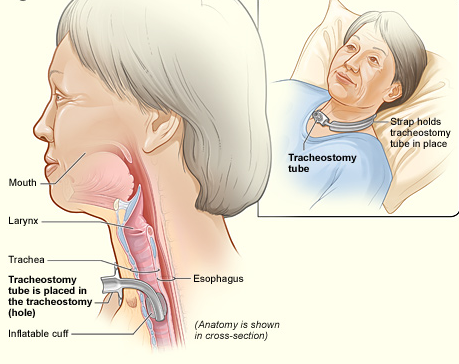
National Heart Lung and Blood Institute (NIH) / Public domain. https://upload.wikimedia.org/wikipedia/commons/e/ed/Tracheostomy_NIH.jpg
He was alive; he was improving; he was starting to thrive.
There I was, talking with physicians about placing a speaking valve on his trach — on a highly contagious, weak, confused, and scared person in the intensive care unit (ICU).
For more info on the Passy Muir® Tracheostomy & Ventilator Swallowing and Speaking Valve (PMV), please see their website (https://www.passy-muir.com). You can find these instructional videos on their homepage and their YouTube channel (search: Passy Muir Educational Animations collection). These make great educational materials for staff covering the ICU these days, who may be new to speaking valves, dysphagia and aspiration issues.
There was no precedent to lean on as this was the first patient in the world that had successfully been able to come off of ECMO and then to very quickly wean off the ventilator.
We discussed dangers of aerosolizing this virus and the risk of potential staff exposure versus the benefit of letting a fellow human being potentially speak with his family for the first time in nearly two months.
Normally, when I would go to place a speaking valve on a person who is post-ECMO (or anyone in the ICU with a trach), there is a long process of preparing that individual for what is about to happen. We educate and attempt to reduce anxiety. We would slowly and completely deflate a cuff and suction. We take a lot of time to check for airflow around the trach tube through the subglottic region (below the vocal cords), through the glottis (aka, vocal cords and noted as larynx in picture above), and out through the pharynx/throat to the nose and mouth. Then we would evaluate with digital (finger) occlusion to check for this airflow. We would involve our otolaryngology team (Ear, Nose and Throat specialists) if we had concerns about restricted airflow, but now their endoscopic evaluations are minimally done during COVID-19. We used to spending lots of time working in the room addressing stress management and diaphragmatic breathing. We would have our colleagues immediately available and/or in the ICU room with us (i.e., respiratory therapist/RT, registered nurse/RN, and others from medical team).
Well, that wasn’t going to be an option in this case as we wanted to limit our time in the room and the number of people in the room. So, it was decided that the RT would stay right outside of the doorway to the room, and myself and the RN would place the valve. That was the decision that was made by the collective team in the moment based on staff availability, but the RT would have also been highly valuable at the bedside.
Here was our process for the speaking valve evaluation:
- Prior to session, he was extensively monitored regarding stability, secretions, his alertness, and ability to participate. In his case, there were no overt contraindications to proceeding with a speaking valve assessment (e.g., no thick copious secretions or frequent suctioning needs).
- A surgical mask was placed over the person’s mouth, as we were changing the airflow. (A speaking valve shunts all the exhaled air out the mouth and nose, so the mouth and nose are new locations for aerosolization).
- I placed the Passy-Muir warning label/sticker on the pilot line of the tracheostomy cuff, as this warns that the cuff must be fully deflated every time before placing the speaking valve on the trach.
- The RN, carefully and slowly deflated the cuff. Suctioning completed with closed circuit.
- The tubing was then detached from the tracheostomy hub.
- We did NOT do digital occlusion/finger occlusion, as our doctors wanted us to disconnect the tubing from the trach hub and pop on the PMV speaking valve as quickly as possible. (This reduces the time that the person is breathing out into the open – to minimize aerosolized particles.)
- I placed the aqua PMV 007 valve directly on the hub of the trach. I felt no back pressure and suspected no airflow resistance. (Performed this quick check, as we cannot do digital occlusion first).
- To then maintain a closed-circuit, I utilized a piece of 6-inch blue corrugated-flexible tubing going from the PMV to the T-piece which then split off in two directions. The one side of tubing was providing supplemental 02, and the second direction of the tubing was connected to a special HME filter (please see picture below). We were prepared with all supplies ahead of time and worked very hard to make the switch quickly to limit any potential for aerosolizing particles. (Note: typically, pre COVID-19, a person would have the speaking valve on the hub of a trach with the trach mask over it.)

We all held our breath.
We all stared expectantly at the patient.
And….. nothing.
I then realized he was waiting for us to speak! So, I asked him how he was feeling. His eyes lit up and he said:
“I’m feeling much better today.”
The RN and I began to laugh and nearly cry all at the same time. He had a voice; he was able to talk to us. He later asked us if we were aliens (because of our PPE)! We were able to get him a device, and he was able to Face Time with his wife.
We all wept that day.
It was in those moments that something profound happened to all of us. We realized there was a glimmer of hope for humanity in this pandemic. We saw life emerge from what was supposed to be guaranteed death. We saw a fellow human survive.
I have always found myself profoundly moved by being the person who first places a speaking valve on a patient and gets to witness them telling their loved ones “I love you” for the first time in a long time. But this moment hit me square in the heart. I realized how important my presence was for this patient and how much he needed me, as an SLP, to be there advocating for him. We are an important part of their short-term survival and long-term quality of life measures.
Later, our team completed a FEES while he was still COVID-19 positive to address his swallowing impairments (after discussing the risks/benefits, documenting our rationale, and in full gear). We got him back to regular foods and thin liquids. With our aggressive weaning team, he was decannulated (trach removal) before he left us.
On Tuesday, April 28, 2020, he left my hospital for a short stay at an acute rehabilitation facility. He will soon be rejoining his family and his life!
*******
Thank you to my guest blogger & hero in this pandemic:
 Jessica Lasky, MS, CCC-SLP, works in Phoenix, Arizona where she runs a mobile FEES company called Mobile Scope. She also works in a neurorehabilitation facility, as well as in a Trauma 1 hospital. She specializes in dysphagia, traumatic brain injury (TBI) and cognition. She is the Vice President of Education for The Dysphagia Outreach Project. In her personal time, she loves going to continuing education opportunities (CEUs) around the country, traveling with her husband, and spoiling her three cats!
Jessica Lasky, MS, CCC-SLP, works in Phoenix, Arizona where she runs a mobile FEES company called Mobile Scope. She also works in a neurorehabilitation facility, as well as in a Trauma 1 hospital. She specializes in dysphagia, traumatic brain injury (TBI) and cognition. She is the Vice President of Education for The Dysphagia Outreach Project. In her personal time, she loves going to continuing education opportunities (CEUs) around the country, traveling with her husband, and spoiling her three cats!
Disclosures:
Jessica Lasky and Karen Sheffler have no financial relationships with companies that provide speaking valves or tracheostomy supplies, such as HMEs.
This patient consented to have his story shared, and he told the SLP that he wanted others to benefit from his story. We thank you for helping others around the world.
*******
Additional Speaking Valve and Tracheostomy
Resources During COVID-19:
by Karen Sheffler, MS, CCC-SLP, BCS-S (updated 6/17/20)
1. National Tracheostomy Safety Project (NTSP at www.tracheostomy.org.uk – website says not secure, but it is legitimate, and they must just not be paying Google for the “https.”): Considerations for tracheostomy in the Covid-19 outbreak:
PDF is secure: https://www.entuk.org/sites/default/files/files/NTSP%20COVID-19%20tracheostomy%20guidance%2020-Mar-2020.pdf
2. Royal College of Speech & Language Therapists (RCSLT):
Webinar 1: COVID-19: Critical Care for SLTs: https://www.rcslt.org/learning/covid-19/rcslt-guidance#section-3
SPEAKERS: Sarah Wallace (consultant SLT, Manchester University, NHS Foundation Trust); Sue McGowan (Clinical Specialist SLT, National Hospital for Neurology and Neurosurgery); and Christina Iezzi (Clinical Lead SLT, Guys and St Thomas’ NHS Foundation Trust).
Topics:
- What is the disease? What do we know? Typical presentations of a patient in the COVID-19 critical care pathway
- How the COVID-19 ICU experience differs from the normal scope of practice • Intubation, post extubation issues
- Tracheostomy management and weaning
3. Thank you to Talia Schwartz, MS, CCC-SLP, from NewYork-Presbyterian/Columbia University Irving Medical Center, for sharing her experience on the front lines in NYC through a blog on Dysphagia Cafe and for providing these insights and resources:
- Global Tracheostomy Collaborative Webinars: https://www.gotostage.com/channel/c4d2288975ce453daf8d9e09860c8da4
- Next Medtronic’s Global Tracheostomy Collaborative webinar on May 5, 2020: Navigating Public Health Crises for Individuals and Families Living with Tracheostomy: COVID-19 and Beyond https://register.gotowebinar.com/register/503603120288385549 (if you miss this one -> it was recorded and will be available. Additionally, there will be more. Follow GTC.)
Resources suggested in that May 5th talk:
-
-
- GTC Website: https://members.globaltrach.org
- Tracheostomy.com
- Connect to the many facebook pages for people with tracheostomies, especially if your supplies are running low. They have connections and support for you.
- Tracheostomy Warriers Support Group Facebook Page – run by Vinciya Pandian, from Johns Hopkins, who is currently working with Dr Martin Brodsky to create consensus materials for working with people who have tracheostomies in these COVID-19 times.
- Dr Robert Graham, MD, of Boston Children’s Hospital and the CAPE Program (CAPE = Critical Care, Anesthesia, Perioperative, Extension (C.A.P.E.) and Home Ventilation Program)
-
- Closed Circuit Suctioning for Trachs: From the UK dubbed “the Kelly Circuit” from creator (who is an RT). https://www.youtube.com/watch?v=PGd5-VhLXcE&feature=youtu.be
4. COVID-19 Passy Muir® Tracheostomy & Ventilator Swallowing and Speaking Valve Webinars and Remote Live In-services. Go to: https://www.passy-muir.com/remote-live-inservices/
In their 4/28/20, they recommended the following resources:
- Sutt, A., Caruana, L.R., Dunster, K.R. et al. Speaking valves in tracheostomised ICU patients weaning off mechanical ventilation – do they facilitate lung recruitment?. Critical Care, 20, 91 (2016). https://doi.org/10.1186/s13054-016-1249-x. Sharable link: https://rdcu.be/b3RLZ
- TRACHTOOLS™ APP
- Evidence-based resources/references on their website.
5. New article June 2020: Speech-Language Pathology Guidance for Tracheostomy During the COVID-19 Pandemic: An International Multidisciplinary Perspective, by Charissa J. Zaga, Vinciya Pandian, Martin B. Brodsky, Sarah Wallace, Tanis S. Cameron, Caroline Chao, et al. (2020). https://pubs.asha.org/doi/pdf/10.1044/2020_AJSLP-20-00089
*******
In Closing:
In addition to thanking our guest blogger, Jessica, I also want to thank to the following speech-language pathologists for sharing their experiences and helping me to start to gather information on this topic: Luis F Riquelme, Talia Schwartz, and Eibhlin Cleary. Talia, in New York City, shared that there were over 60 people with tracheostomies at her hospital last week. Clinicians around the US are preparing. I encourage others to send more info and resources.
Eibhlin put it well, noting how we are all sharing anecdotal experience, rather than specific advice based on evidence. Evaluating and treating under these conditions is new. As Dr Riquelme stated, without instrumental evaluations and endoscopies, we are all a “bit blind.” We are doing our best for people with our available evidence and critical thinking. Thank you also to the therapists on the RCSLT talk noted above for your global leadership: Sarah Wallace, Sue McGowan and Christina Iezzi.
Many SLPs/SLTs that I have talked with an on webinars have reported similarly waiting until the person with COVID-19 is ventilator-free before trying cuff deflation and speaking valve placement on the trach. Many note the need to avoid finger occlusion and the use of a T-piece with closed-circuit suction and with HME. They warned that all of this is aerosolizing and adequate PPE is essential (see article linked above with photo of the Phoenix team). The infectious disease specialist at Jessica’s hospital stated that a person may be COVID-19 positive for up to a month after discharge. Eibhlin noted how co-treating with physical therapy/physiotherapy has been helpful. Eibhlin also admitted that once these people with COVID-19 “turn the corner,” they have so far been easier to wean and can tolerate the speaking valve better than many of the neurologically impaired individuals she has worked with in the past. (Those with COVID-19 who don’t turn the corner and who cannot wean from the ventilator are going to long-term acute care/LTAC with gastrostomy feeding tubes in place, per Talia.)
SLPs like to remind the medical team that even though these devices are called speaking valves, they are really one-way valves that help with: smell, taste, cough, restoring subglottic pressure, improving the safety of the swallow, and secretion management to reduce need for suctioning. (Not to mention the psychosocial benefits of communicating). The speaking valves have helped her patients with secretion management so that they can work towards decannulation, per Eibhlin.
More to come.
Please share in the comments below. We are #InThisTogether!