
Oral Health: 3 International Updates & Actions
by Karen Sheffler, MS, CCC-SLP, BCS-S inspired by the Dysphagia Research Society (DRS) Annual Conference in Philadelphia, PA & the session on March 28, 2025 titled: “Raising the Profile of Dysphagia on the Oral Health Research and Access Agenda.”

The international perspectives at the Dysphagia Research Society is always inspiring!. There were 27 countries that came together to advance the science of swallowing at this year’s meeting. This article will cover oral health updates and resources from 3 terrific speakers: Dr. Paul Allison, Ms. Shauna Hachy, and Dr. Kiochiro Matsuo. The session was moderated by Dr. Rebecca Affoo, PhD, CCC-SLP, SLP-Reg, SLP(C) of Dalhousie University, Canada and the Oral Health & Swallowing Research Lab. I have written about oral hygiene, oral health, and oral infection control many times over the years, so I am very excited to share these 2025 updates!
1. Oral Health Collaboration Across Canada with NOHRS
Dr. Paul Allison, faculty of Dental Medicine and Oral Health Sciences at McGill University, presented at DRS on how dysphagia must fit into new national oral health strategies.
Dr. Allison inspired this international audience by sharing the years of work of NOHRS (The Canadian National Oral Health Research Strategy). NOHRS is an essential collaboration in Canada among the following organizations:
- Canadian Institute of Health Research (CIHR or IRSC in French and is the Canadian equivalent to the NIH in the US) with its institute that supports oral health is the Institute of Musculoskeletal Health and Arthritis,
- Canadian Dental Association,
- Network for Canadian Oral Health Research,
- Canadian Dental Therapists Association (CDTA),
- Association of Canadian Faculties of Dentistry (ACFD),
- Canadian Dental Hygienists Association, and the
- Canadian Association for Dental Research (CADR).
Dr. Allison pointed out 2 international commissions that partially informed this Canadian oral health research strategy (see my recommended action plan and reference section at the end of this article for more information on these projects):
- The WHO Global Strategy and Action Plan on Oral Health for 2023-2030, which was published in 2024;
- The Lancet Commission on Oral Health, who have published a series of statements since 2019 and will publish a full report this year (2025).
He urged the Dysphagia Research Society (DRS) to become involved in these Canadian and international efforts. We must incorporate dysphagia into these oral health strategies. However, he warned that it cannot be only be the professional associations supporting it, as a movement like this needs the backing of the relevant governmental research funding agencies. The topic of dysphagia needs to be included across many commissions/global action plans, as dysphagia is not a disease in-and-of-itself. Dysphagia is a symptom of many different chronic diseases, disorders, and structural or functional differences. The negative sequelae (immediate and long-term effects) of dysphagia are varied, such as: aspiration, pneumonia, choking, malnutrition, dehydration, exacerbation of underlying diseases, and death. When risks of these negative sequelae can be reduced through actions to improve oral health across a population, that should be the time to act at all levels.
Canada is leading the way with NOHRS in discussing important issues of access to oral health care and the inequities in care. The NOHRS wants to “galvanize the community and leverage our strengths,” according to Dr. Allison, to meet the following goals:
- Improve oral health & reduce inequities in Canada;
- Improve oral research capacity in Canada.
Here is great summary article by NOHRS co-chairs: Dr. Leigha Rock and Dr. Paul Allison. See links to the full NOHRS document on the Oral Health Initiative here. As you can see in the NOHRS website, the Oral Health Data Platform collaborated with Statistics Canada to survey in order to determine knowledge gaps and guide future research in the following areas:
- “Social determinants, inequalities and inequities in oral health and disease, oral health care and associated impacts across Canada;
- The oral microbiome, oral inflammation and systemic health, including nutritional status;
- The relationship between dental treatments and systemic health.”
He stressed that Implementation Science is a big priority. Implementation science for oral health does not simply point out the gaps in oral health equity. It reaches out and includes communities, builds networks, and collaborates directly with patient-groups and community groups (e.g., aging communities, rural communities, indigenous communities, etc). He noted that dysphagia can easily fit into all goals and priorities.
Dr. Paul Allison is involved with NOHRS as well as The Lancet Commission on Oral Health. He hopes to collaborate further with dysphagia clinicians and researchers. (See all Lancet Commission on Oral Health members here.)
Get inspired and add this collaboration opportunity to your dysphagia advocacy to-do lists!
Keep reading, as update #2 is a great example of this Implementation Science, putting oral health knowledge into action.
The update #3 is a real treat with many resources from Dr. Matsuo, who has been a global leader in oral health for many years.
2. Oral Health Example from an Indigenous Community
We were fortunate to immediately hear an example of implementation science when Shauna Hachey shared her session on: “Oral health across the lifespan: Examples of mobilizing knowledge through interprofessional collaboration. Bridging Research and Practice.” Ms. Hachey is an Associate Professor at Dalhousie Faculty of Dentistry, School of Dental Hygiene. She demonstrated community-led partnerships with the Mi’kmaq community to create a children’s book promoting oral health. The Mi’kmaq Indigenous / First Nation people live in the territory of Mi’kma’ki that extends from northeastern Maine to Canada’s Atlantic provinces (Nova Scotia, New Brunswick, Prince Edward Island, parts of Newfoundland), and the Gaspé Peninsula of Quebec. Learn more about this community’s stories and the Baby Smiles Dental Health project and book: Baby Smiles: Weskewikwa’sit mijua’ji’j. Project by: Tui’kn Partnership with illustrations by Loretta Gould.
Shauna Hachey noted:
“Oral health improves with behavioral change. Implementation science, providing the knowledge and tools to enable behavioral change, can make a difference.”
Ms. Hachey recommended an online comprehensive oral hygiene toolkit called: Brushing Up on Mouth Care (www.brushingup.ca). Ms. Hachey acknowledged the work by Dr. Mary McNally and the Brushing Up team. This website provides a host of open access resources that were developed as part of a research project at Dalhousie University (Halifax, Nova Scotia). The research and website are also supported through Healthy Populations Institute (HPI), a research institute at Dalhousie University.
Read on to find where Dr. Matsuo recommends the Oral Health Assessment Tool (OHAT) for healthcare providers. Brushing Up on Mouth Care created a free YouTube video to train this tool. Thank you!
3. Japanese Oral Health Recommendations & Research
The Japanese experience was presented by Dr. Koichiro Matsuo, of the Oral Health Sciences for Community Welfare Institute of Science, Tokyo and the Oral Health Center, Institute of Science Tokyo (IST Hospital). He emphasized that before one can evaluate swallowing, you need to assess the person’s oral health status. He stressed that typically in “medically compromised patients, oral health is also compromised.”
Poor oral health leads to:
- poor oral hygiene,
- cavities,
- missing dentition,
- dentures with many problems,
- a lack of dentures,
- dry mouth, and even
- poor oral sensorimotor function and strength.
He divided his talk into two categories of interest: oral hygiene and oral function.
Oral Hygiene
When nurses discuss cleaning the mouth in the United States, they often use the term “oral care.” However, that phrase is not strong enough. Poor oral health leads to a biofilm build-up on the surfaces of the teeth, all mucous membranes, and dentures. Dr. Matsuo warned that the surface of dentures can become easily contaminated due to the artificial material that can trap food and harbor bacteria in microscopic cracks and rough spots. Many kinds of bacteria (not simply staphylococcus aureus; read more here) are found in the oral cavity, saliva, and sputum of individuals with aspiration pneumonia. The pneumonia is caused by an inhalation of bacteria in saliva and of liquid/foods that have been contaminated with these bacteria. Poor oral health does not only cause aspiration pneumonia; it also causes endocarditis, respiratory diseases, gastrointestinal infections, and more. See selected references from Dr. Matsuo’s talk at the end of this article that support this discussion.
OHAT
According to Dr. Matsuo, in order to stress the importance of systematic oral care, we need a screening tool that can be used across all disciplines, unifies terminology, and creates good communication and quick referrals. He uses the OHAT (Oral Health Assessment Tool), originally from Chalmers and colleagues in 2005. Now the OHAT has been translated and validated in many languages around the world (see references below). It is a fairly easy one-page chart of 8 oral health categories (lips, tongue, gums/tissue, saliva, natural teeth, dentures, oral cleanliness, and dental pain). The screener rates 0 for healthy to 1 as notable changes to 2 for unhealthy. The healthcare provider takes action (interventions on site or via referrals – see pink highlighted sections) if concerning changes (1) are noted. Whereas, a rating of 2 always requires a referral to an oral health professional. It is terrific that the bottom of the OHAT form guides the multidisciplinary communication, but I would of course add the speech-language pathologist (SLP) to the list of referral options, along with those disciplines such as dietitian and occupational therapy (OT) already on the list. Medication review is also extremely important as medication side-effects can cause dry mouth and other unintended dysphagia (iatrogenic dysphagia).
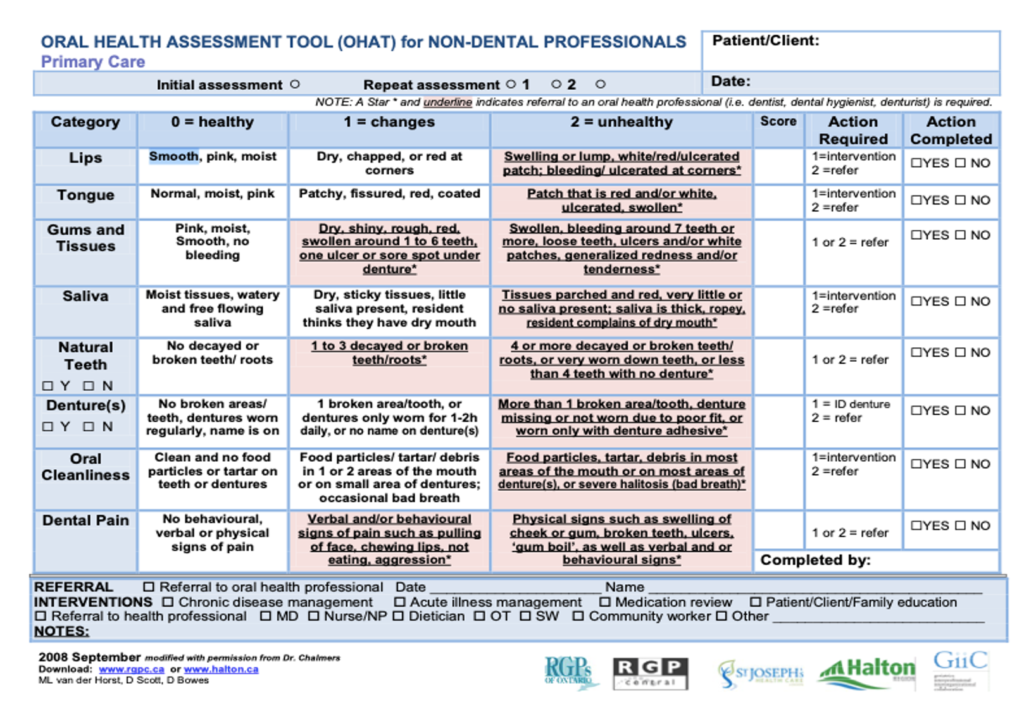
Oral Health Assessment Tool (OHAT) in English. A chart of 8 items to help healthcare providers screen oral health with ratings of 0, 1, 2, with the rating of 2 always requiring a referral to a oral health professional.
Oral Health Assessment Tool (OHAT) instructional video and links can be found on BrushingUp.ca here and on YouTube. Thanks again to HPI and Dalhousie University’s research and resources, such as this Brushing Up on Mouth Care education series.
Please also see a pdf of the Oral Health Assessment Tool (OHAT) translated into Japanese, as it provides good photos within the chart to guide the ratings for each of the 8 items.
Dr. Matsuo took this a step further and studied the associations among oral intake, oral function, and oral health, especially looking at post-stroke management in the acute through subacute time periods. See the 2024 studies cited below by Sekimoto and colleagues, as well as Sakai and colleagues. They found that with direct dental interventions, there was improvement in oral health, which contributed to improvements in oral function and oral intake. It is truly inspirational that Japan’s rehabilitation centers can have such a huge impact on people’s oral health during long stays of 60-90 days after a stroke. They coordinate care and provide general oral health interventions, tooth extractions, periodontal treatment, denture repair, denture fabrication, and more — all during a rehab stay!
Oral Function
Poor oral health can lead to poor oral function. When Dr. Matsuo discussed this connection, he mentioned a phrase that was new to me:
Oral Frailty
A new hot topic. The phrase initially came from a working group in Japan in 2014!
Oral frailty makes sense. Dr. Matsuo walked us through the connections. Having poor oral health and fewer teeth may make you avoid harder foods, like meats and vegetables. You may reduce the variety of foods you take in, causing your nutritional balance to be off. You may be eating the same amount of calories as someone with healthy teeth, but your diet may have more carbohydrates and fats, rather than enough proteins and vitamins. That could lead to under-nutrition, which leads to frailty, falls, fractures, infections, and decline. Alternatively, due to higher carbohydrates and fats, it could lead to over-nutrition and unhealthy weight gain, which may increase risks for stroke, diabetes, and heart disease. Both of these paths lead to more risks for needing long-term nursing care. He cited several studies that connect decreased number of teeth with malnutrition (Yoshihara et al., 2005; Wakai et al., 2010; Inui et al., 2017; Toniazzo et al., 2017).
He referred to a systematic review by Dibello and colleagues from Italy (2021). This study organized 39 articles regarding oral function into 4 categories that may be associated with the onset of oral frailty:
- Oral pain (tooth or mouth pain)
- Oral health status deterioration
- Oral dysbiosis (another important phrase to add to your vocabulary, meaning an altered microbiome that can cause serious oral and systemic health problems. I wrote about this shift in the microbial community in people in critical care here, where I compared the biome shift after a volcano to the microbiome shift with the stress and environmental factors affecting institutionalized/hospitalized adults.)
- Periodontal disease
- Oral health
- Number of teeth
- Chewing, swallowing and saliva disorders
- Difficulty chewing
- Difficulty swallowing
- Dry mouth
- Deterioration of oral motor skills
- Oral diadochokinesis (i.e., pa, ta, ka repetitions as fast as you can, called DDK rate)
- Tongue pressure
- Occlusal force
- Masticatory function
Dr. Matsuo reported that the consensus statement on oral frailty is (Tanaka et al., 2024):
“Oral frailty is a state between robust oral function (a “healthy mouth”) and its decline, characterized by slight declines in oral function, including tooth loss and difficulties in eating and communicating, which increase the risk of impaired oral functional capacity but can be reversed with proper intervention and treatment. Oral frailty can be assessed using the Oral Frailty 5‐item Checklist (OF‐5) without the need for a dental health professional. Oral frailty is defined as having at least two of the following components: (i) fewer teeth, (ii) difficulty chewing, (iii) difficulty swallowing, (iv) dry mouth, and (v) low articulatory oral motor skills. Approximately 40% of community‐dwelling older adults have oral frailty. Oral frailty is associated with poor dietary variety, social isolation, physical frailty, disability, and mortality.”
Oral Frailty 5-Item Checklist (OF-5)
Tanaka and team (2023) created an “Oral Frailty 5-item Checklist.” The global society appreciates these open access publications!
In this OF-5 screening tool, if the person says “YES” to at least 2 out of 5, they are at risk for oral frailty and in need of further nursing interventions. Tanaka and team studied over 2000 community-dwelling older adults and found that if they scored a 2 or more, they had a significantly increased rate of having physical frailty. When a person has both oral frailty and physical frailty, there is a significantly higher risk for nursing care, physical disability, and mortality. See the consensus statement on oral frailty by Tanaka and colleagues (2024), which notes that increased awareness is essential to detect the early signals of these “slight” declines. You can see the educational diagrams they created for healthcare professionals and the public. Performing this Oral Frailty 5-Item Checklist at routine healthcare and dental visits would be one first-step preventative action. This simple actions can reduce the risks of further decline into frailty, sarcopenia (muscle wasting/muscle loss), malnutrition/under-nutrition, and death.
| Concept | Task/Question | Yes = 1 Oral Frailty Point |
| 1. Fewer teeth | How many of your natural teeth are left? (count) | <20 = yes (0-19 teeth) |
| 2. Difficulty chewing | Do you have difficulty chewing tough foods now compared with 6 months ago? | Yes / No |
| 3. Difficulty swallowing | * Do you have difficulty swallowing, feel foods get stuck in your mouth/throat, and/or cough with your liquids and foods recently? (question modified for clarity from “Have you choked on your tea or soup recently?”) | Yes / No |
| 4. Dry mouth | Do you often have dry mouth? | Yes / No |
| 5. Low articulatory oral motor skills | Do you have difficulty with clear pronunciation recently? Therapist: Test diadochokinesis/DDK with rapid repetition of the “ta” sound. | Ability to do:
<6 times per second or <30 times per 5 seconds. See website: www.ohcw-tmd.com for a tool to help count these. |
| TOTAL |
* Question #3 modified by Karen Sheffler, MS, CCC-SLP, BCS-S SwallowStudy.com |
2 or more out of 5 = FRAILTY |
I modified the swallowing difficulty question in #3 below as noted in this chart, as one does not “choke” on tea since it does not block the airway or asphyxiate a person.
*******
Summary on Oral Health Actions
The mouth is forgotten in healthcare, as I outlined in my article years ago, which is surprising as it is the largest hole in the body where infectious material can enter! All healthcare providers can play a role in screening people for poor oral health to prevent the many negative sequelae such as poor oral function, dysphagia, aspiration pneumonia, choking, and even early death. It is easy to get started with oral health screening tools like the OHAT and OF-5.
Oral health is also found to be crucial in Dementia prevention. See Dr. Xiang Qi’s statements in this informative Q&A article urging The Lancet Commission on Dementia to consider oral health risk factors. Out of the 14 risk factors for Dementia, why was oral health overlooked? See Oral health is a Crucial Overlooked Risk Factor for Dementia, where Dr. Xiang Qi states:
“First, recognize oral health as a potential risk factor when assessing patients’ overall dementia risk profile. Include questions about oral hygiene practices, tooth loss, periodontal disease and dental care access in patient assessments.
Second, emphasize preventive dental care for all patients, particularly those with other dementia risk factors.”
When I key-word searched the WHO Global Strategy & Action Plan on Oral Health 2023 – 2030 (2024), I noted that it does not mention “aspiration,” “dysphagia,” or “choking.” Fortunately, the WHO did connect poor oral health with pneumonia with these statements:
“…Concerned about the effect of poor oral health on quality of life and healthy aging both physically and mentally; and noting that poor oral health is a regular cause of pneumonia for elderly people, particularly those living in care facilities, and for persons with disabilities;
Aware that poor oral health is a major contributor to general health conditions, and noting that it has particular associations with cardiovascular diseases, diabetes, cancers, pneumonia and premature birth;…” (section titled: “Annex 2: World health assembly Resolution on oral health WHA74.5,” page 85-87)
However, this WHO report only mentioned “swallowing” one time, and not in a context of aspiration pneumonia. This was in the section called: Overarching goal targets, Section B on Reduced Oral Disease Burden. Section B.10 has a chart titled Self-Reported Oral Health Status (page 65 details as follows).
- Indicator Definition: “Percentage of population who reported a problem, including functional limitation, because of the state of their teeth, gums or mouth. Problems include but are not limited to:
- difficulty in chewing foods
- difficulty in swallowing water
- difficulty with speech or trouble pronouncing words
- mouth feeling dry
- avoiding smiling
- days not at work or school because of teeth or mouth.”
Do you see problems with this WHO list and with the idea that it is the only location in an 80+ page report that refers to difficulty swallowing?
First, self-reported data cannot be the only method they are using to reduce disease burden. We know that dysphagia often goes under-reported due people not being aware of their swallowing problem. Often, there are silent safety and efficiency issues (i.e., silent aspiration of material going down the wrong way that you do not sense and residue that you do not feel in throat and/or esophagus). It is important for these screening tools to trigger appropriate referrals for more comprehensive dysphagia evaluations by the SLP that test food, liquids, and pills in a multiphase dysphagia evaluation. Instrumental evaluations by the SLP can help guide your treatment plan. The SLP can then make appropriate referrals to neurology, otolaryngology, and gastroenterology as needed.
Second, if you are having significant functional limitations in your mouth, you are most likely to have difficulty swallowing solid foods (not just liquids as the list indicates). The list does include difficulty chewing. Therefore, if you have poor oral health, difficulty chewing, and dry mouth, it is highly probable that food will get stuck in your mouth, throat, and/or esophagus. Poor chewing and dry mouth can lead to difficulties with the food clearing through the esophageal and may cause esophageal retention, food impaction, and regurgitation.
When dysphagia is left out of important global strategy action plans, we are missing opportunities for lifesaving warnings. Let us continue to advocate for dysphagia awareness, as this life-threatening symptom has long gone under-reported, under-evaluated, under-treated, and under-funded.
Three ACTION ITEMS for Oral Health & Dysphagia
- Include oral health in general medicine and preventative medicine.
- Advocate for swallowing issues to be a part of global strategic plans for oral health.
- Screen early and often to make appropriate referrals to speech pathologists and others who evaluate and manage dysphagia.
*******
Prior Oral Infection Control/Aspiration Precautions Blogs on SwallowStudy.com:
- Oral Care & Aspiration Pneumonia Prevention
- 10 Trillion Microorganisms vs Your Toothbrush (Part I: Oral Hygiene)
- What Do Volcanoes & Mouths Have in Common? (Part II: Oral Microbiome & Saliva where I discuss the saliva and salivary pH by comparing the mouth of a critically ill person to the disturbance of the ecosystem after Mount Saint Helen’s volcano.)
- Take a Trip to the Lungs with 12 Bacterial Species (Part III: Oral Hygiene where I discuss the many pathogens that may colonize the mouth and take a trip it into the lungs).
- How To Perform Effective Oral Care (Part IV). Read more on Chlorhexidine, Hydrogen Peroxide and how to provide good oral infection control.
- It’s Alive! Oral Microbiome (Where I compare the delicate microbiome of the mouth to that of a dessert!)
- Saliva Puzzle: Saliva Production & Swallowing
- Please see my March 25, 2021 webinar hosted by the National Foundation of Swallowing Disorders (NFOSD) titled: More Than Oral Care – Let’s Talk Oral Infection Control
- See also an important article on choking risks: Bread of Life? Evidence on Choking Risks with Bread
- Because chemoradiation exposure during head and neck cancer treatment greatly affects the mouth and oral health, here is further reading on that.
Thank you as always for reading, commenting, & sharing to raise awareness!
References & Resources:
The Lancet Commission on Oral Health, formed 2019
The Lancet Series on Oral Health 2019: https://www.thelancet.com/series/oral-health ~ Full report by this commission due out in 2025.
Watt, R. G., Daly, B., Allison, P., Macpherson, L. M. D., Venturelli, R., Listl, S., Weyant, R. J., Mathur, M. R., Guarnizo-Herreño, C. C., Celeste, R. K., Peres, M. A., Kearns, C., & Benzian, H. (2019). Ending the neglect of global oral health: time for radical action. Lancet (London, England), 394(10194), 261–272. https://doi.org/10.1016/S0140-6736(19)31133-X
Peres, M. A., Macpherson, L. M. D., Weyant, R. J., Daly, B., Venturelli, R., Mathur, M. R., Listl, S., Celeste, R. K., Guarnizo-Herreño, C. C., Kearns, C., Benzian, H., Allison, P., & Watt, R. G. (2019). Oral diseases: a global public health challenge. Lancet (London, England), 394(10194), 249–260. https://doi.org/10.1016/S0140-6736(19)31146-8
Livingston, G., Huntley, J., Liu, K. Y., Costafreda, S. G., Selbæk, G., Alladi, S., Ames, D., Banerjee, S., Burns, A., Brayne, C., Fox, N. C., Ferri, C. P., Gitlin, L. N., Howard, R., Kales, H. C., Kivimäki, M., Larson, E. B., Nakasujja, N., Rockwood, K., Samus, Q., … Mukadam, N. (2024). Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet (London, England), 404(10452), 572–628. https://doi.org/10.1016/S0140-6736(24)01296-0
Summary of this Lancet Commission on Dementia’s 14 Risk Factors:
https://www.healio.com/news/psychiatry/20240731/eliminating-14-risk-factors-may-prevent-nearly-half-of-dementia-cases
WHO Global Strategy & Action Plan in Oral Health ~ 2023 – through 2030
WHO Citation: Global strategy and action plan on oral health 2023–2030. Geneva: World Health Organization; 2024. Licence: CC BY-NC-SA 3.0 IGO.
https://www.who.int/news/item/26-05-2024-who-releases-global-strategy-and-action-plan-on-oral-health
Download Plan here (this contains key documents that “inform and define the renewed global oral health agenda towards 2030”): https://www.who.int/publications/i/item/9789240090538
Ben Yahya I. (2024). Global oral health initiative: World Health Organization strategic action plan. Journal of dental education, 88 Suppl 1, 699–702. https://doi.org/10.1002/jdd.13504
Selected Dr. Matsuo References ~ Oral Hygiene & Oral Function:
Adachi, M., Ishihara, K., Abe, S., & Okuda, K. (2007). Professional oral health care by dental hygienists reduced respiratory infections in elderly persons requiring nursing care. International journal of dental hygiene, 5(2), 69–74. https://doi.org/10.1111/j.1601-5037.2007.00233.x
Alzamil, H., Wu, T. T., van Wijngaarden, E., Mendoza, M., Malmstrom, H., Fiscella, K., Kopycka-Kedzierawski, D. T., Billings, R. J., & Xiao, J. (2021). Removable Denture Wearing as a Risk Predictor for Pneumonia Incidence and Time to Event in Older Adults. JDR clinical and translational research, 8(1), 23800844211049406. Advance online publication. https://doi.org/10.1177/23800844211049406
Awano, S., Ansai, T., Takata, Y., Soh, I., Akifusa, S., Hamasaki, T., Yoshida, A., Sonoki, K., Fujisawa, K., & Takehara, T. (2008). Oral health and mortality risk from pneumonia in the elderly. Journal of dental research, 87(4), 334–339. https://doi.org/10.1177/154405910808700418
Coulthwaite, L., & Verran, J. (2007). Potential pathogenic aspects of denture plaque. British journal of biomedical science, 64(4), 180–189. https://doi.org/10.1080/09674845.2007.11732784
Dibello, V., Zupo, R., Sardone, R., Lozupone, M., Castellana, F., Dibello, A., Daniele, A., De Pergola, G., Bortone, I., Lampignano, L., Giannelli, G., & Panza, F. (2021). Oral frailty and its determinants in older age: a systematic review. The lancet. Healthy longevity, 2(8), e507–e520. https://doi.org/10.1016/S2666-7568(21)00143-4
Hannah, V. E., O’Donnell, L., Robertson, D., & Ramage, G. (2017). Denture Stomatitis: Causes, Cures and Prevention. Primary dental journal, 6(4), 46–51. https://doi.org/10.1308/205016817822230175
Iinuma, T., Arai, Y., Abe, Y., Takayama, M., Fukumoto, M., Fukui, Y., Iwase, T., Takebayashi, T., Hirose, N., Gionhaku, N., & Komiyama, K. (2015). Denture wearing during sleep doubles the risk of pneumonia in the very elderly. Journal of dental research, 94(3 Suppl), 28S–36S. https://doi.org/10.1177/0022034514552493
Inui, A., Takahashi, I., Kurauchi, S., Soma, Y., Oyama, T., Tamura, Y., Noguchi, T., Murashita, K., Nakaji, S., & Kobayashi, W. (2017). Oral conditions and dysphagia in Japanese, community-dwelling middle- and older- aged adults, independent in daily living. Clinical interventions in aging, 12, 515–521. https://doi.org/10.2147/CIA.S132637
Matsuo, H., Yoshimura, Y., Fujita, S., Maeno, Y., & Tanaka, S. (2023). Association of poor oral health with increased incidence of dysphagia and impaired improvement in nutritional status among patients with acute heart failure: a prospective cohort study. European geriatric medicine, 14(4), 879–888. https://doi.org/10.1007/s41999-023-00810-0
O’Donnell, L. E., Smith, K., Williams, C., Nile, C. J., Lappin, D. F., Bradshaw, D., Lambert, M., Robertson, D. P., Bagg, J., Hannah, V., & Ramage, G. (2016). Dentures are a Reservoir for Respiratory Pathogens. Journal of prosthodontics : official journal of the American College of Prosthodontists, 25(2), 99–104. https://doi.org/10.1111/jopr.12342
Ortega, O., Parra, C., Zarcero, S., Nart, J., Sakwinska, O., & Clavé, P. (2014). Oral health in older patients with oropharyngeal dysphagia. Age and ageing, 43(1), 132–137. https://doi.org/10.1093/ageing/aft164
Takeshita, T., Suzuki, N., Nakano, Y., Shimazaki, Y., Yoneda, M., Hirofuji, T., & Yamashita, Y. (2010). Relationship between oral malodor and the global composition of indigenous bacterial populations in saliva. Applied and environmental microbiology, 76(9), 2806–2814. https://doi.org/10.1128/AEM.02304-09
Takeshita, T., Tomioka, M., Shimazaki, Y., Matsuyama, M., Koyano, K., Matsuda, K., & Yamashita, Y. (2010). Microfloral characterization of the tongue coating and associated risk for pneumonia-related health problems in institutionalized older adults. Journal of the American Geriatrics Society, 58(6), 1050–1057. https://doi.org/10.1111/j.1532-5415.2010.02867.x
Tanaka, T., Hirano, H., Ikebe, K., Ueda, T., Iwasaki, M., Shirobe, M., Minakuchi, S., Akishita, M., Arai, H., & Iijima, K. (2023). Oral frailty five-item checklist to predict adverse health outcomes in community-dwelling older adults: A Kashiwa cohort study. Geriatrics & gerontology international, 23(9), 651–659. https://doi.org/10.1111/ggi.14634
Tanaka, T., Hirano, H., Ikebe, K., Ueda, T., Iwasaki, M., Minakuchi, S., Arai, H., Akishita, M., Kozaki, K., & Iijima, K. (2024). Consensus statement on “Oral frailty” from the Japan Geriatrics Society, the Japanese Society of Gerodontology, and the Japanese Association on Sarcopenia and Frailty. Geriatrics & gerontology international, 24(11), 1111–1119. https://doi.org/10.1111/ggi.14980 https://pubmed.ncbi.nlm.nih.gov/39375858/
Toniazzo, M. P., Amorim, P. S., Muniz, F. W. M. G., & Weidlich, P. (2018). Relationship of nutritional status and oral health in elderly: Systematic review with meta-analysis. Clinical nutrition (Edinburgh, Scotland), 37(3), 824–830. https://doi.org/10.1016/j.clnu.2017.03.014
Wakai, K., Naito, M., Naito, T., Kojima, M., Nakagaki, H., Umemura, O., Yokota, M., Hanada, N., & Kawamura, T. (2010). Tooth loss and intakes of nutrients and foods: a nationwide survey of Japanese dentists. Community dentistry and oral epidemiology, 38(1), 43–49. https://doi.org/10.1111/j.1600-0528.2009.00512.x
Yoshihara, A., Watanabe, R., Nishimuta, M., Hanada, N., & Miyazaki, H. (2005). The relationship between dietary intake and the number of teeth in elderly Japanese subjects. Gerodontology, 22(4), 211–218. https://doi.org/10.1111/j.1741-2358.2005.00083.x
Matsuo’s References Related to OHAT:
ORIGINAL: Chalmers, J. M., King, P. L., Spencer, A. J., Wright, F. A., & Carter, K. D. (2005). The oral health assessment tool–validity and reliability. Australian dental journal, 50(3), 191–199. https://doi.org/10.1111/j.1834-7819.2005.tb00360.x https://pubmed.ncbi.nlm.nih.gov/16238218/
OHAT is a modification of the Brief Oral Health Status Examination (BOHSE):
Chen C. C. (2009). The Kayser-Jones Brief Oral Health Status Examination (BOHSE). ORL-head and neck nursing : official journal of the Society of Otorhinolaryngology and Head-Neck Nurses, 27(2), 14–15.
PORTUGUESE: Cerveira, F. R., Matos, M. A. C., & Sa-Couto, P. (2022). Development of the European Portuguese version of the oral health assessment tool: Content validity and reliability study in an elderly population. Special care in dentistry : official publication of the American Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry, 42(6), 623–629. https://doi.org/10.1111/scd.12724
JAPANESE: Matsuo, K. & Nakagawa, K. (2016). Reliability and validity of the Japanese version of oral health assessment tool (OHAT-J) [Japanese]. Journal Japanese Society Disability Oral Health, 37, 1-7. See website page: https://www.ohcw-tmd.com/research/ohat.html
- In Japanese – See pdf.
- In Japanese – See YouTube instructional video (terrific pictures demonstrating ratings of 0, 1, 2 in each OHAT category):
SPANISH (study from Chile): Morales, C., Henríquez, F., & Muñoz, S. (2023). Structural validity and reliability of the “Oral Health Assessment Tool” applied by speech-language therapists in a population of older Chilean people. BMC oral health, 23(1), 24. https://doi.org/10.1186/s12903-023-02725-5
GERMAN: Klotz, A. L., Zajac, M., Ehret, J., Hassel, A. J., Rammelsberg, P., & Zenthöfer, A. (2020). Development of a German version of the Oral Health Assessment Tool. Aging clinical and experimental research, 32(1), 165–172. https://doi.org/10.1007/s40520-019-01158-x
BELGIUM study: Simpelaere, I. S., Van Nuffelen, G., Vanderwegen, J., Wouters, K., & De Bodt, M. (2016). Oral health screening: feasibility and reliability of the oral health assessment tool as used by speech pathologists. International dental journal, 66(3), 178–189. https://doi.org/10.1111/idj.12220
CHINESE study: Tian, F., Li, J., Wu, B., Xiao, R., Liu, J., Yu, J., Liu, L., & Zhu, R. (2023). Differences in the oral health status in hospitalised stroke patients according to swallowing function: A cross-sectional study. Journal of clinical nursing, 32(7-8), 1140–1147. https://doi.org/10.1111/jocn.16254 (OHAT has been validated in Chinese, and this study used OHAT scoring in a Chinese study)
Matsuo’s References on Oral Health & Stroke
Aoyagi, M., Furuya, J., Matsubara, C., Yoshimi, K., Nakane, A., Nakagawa, K., Inaji, M., Sato, Y., Tohara, H., Minakuchi, S., & Maehara, T. (2021). Association between Improvement of Oral Health, Swallowing Function, and Nutritional Intake Method in Acute Stroke Patients. International journal of environmental research and public health, 18(21), 11379. https://doi.org/10.3390/ijerph182111379
Eto, F., Nezu, T., Nishi, H., Aoki, S., Tasaka, S., Horikoshi, S., Yano, K., Kawaguchi, H., & Maruyama, H. (2024). Oral condition at admission predicts functional outcomes and hospital-acquired pneumonia development among acute ischemic stroke patients. Clinical oral investigations, 28(8), 434. https://doi.org/10.1007/s00784-024-05833-w
Matsuo, K., Sekimoto, Y., Okamoto, M., Shibata, S., & Otaka, Y. (2022). Association between oral health status and oral food intake level in subacute stroke patients admitted to a convalescent rehabilitation unit. Gerodontology, 39(1), 67–73. https://doi.org/10.1111/ger.12586
Sakai, A., Matsuo, K., Sekimoto, Y., Hidaka, R., & Yoshihara, A. (2024). Changes in oral health status with dental intervention during the acute to subacute stages of stroke. Gerodontology, 41(2), 276–282. https://doi.org/10.1111/ger.12706
Sekimoto, Y., Matsuo, K., Sakai, A., Shibata, S., & Minakuchi, S. (2024). Improvement of oral function and its impact on oral food intake in subacute stroke patients: A prospective study with dental intervention. Journal of oral rehabilitation, 51(8), 1365–1372. https://doi.org/10.1111/joor.13711