
Obstructive Sleep Apnea (OSA) & Dysphagia
Guest Writers & Researchers in Obstructive Sleep Apnea and Dysphagia: Ankita M. Bhutada, PhD; Emma Wallace, PhD and Kendrea L. Focht (Garand), PhD, CScD, CCC-SLP, BCS-S, CBIS, CCRE
Editor: Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction to Obstructive Sleep Apnea (OSA)
Obstructive sleep apnea is a sleep-related breathing disorder affecting around 1 billion worldwide (Benjafield et al., 2019). Untreated OSA is often associated with a myriad of complex fatal conditions, such as:
- cardiovascular accidents,
- stroke,
- pulmonary disorders, and
- neurocognitive sequelae.
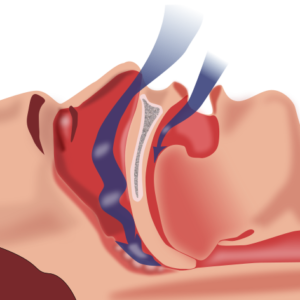
Physiologic Risk Factors in Obstructive Sleep Apnea. (Image downloaded & used with permission by Habib M’henni, User:Dyolf77, Wikimedia Commons, 2/8/23)
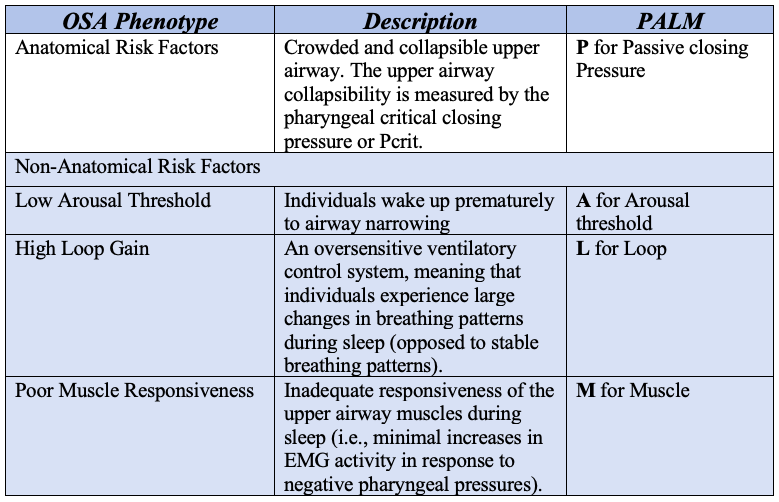
In addition, OSA often occurs with other conditions, such as spinal cord injury, multiple sclerosis, and Parkinson’s disease (Adler & Janssens, 2018; Jehan et al., 2019; Tietjens et al., 2019). The pathophysiology of OSA is complex, and one way to classify OSA is with these four major pathophysiologic phenotypes, including (Eckert & Malhotra, 2008; Carberry et al., 2016; Zinchuk et al., 2017):
- Anatomical risk factors resulting in a crowded upper airway, and non-anatomical risk factors such as:
- Low arousal threshold,
- High loop gain, and
- Poor muscle responsiveness.
The chart below simplifies and briefly describes these phenotypes. The use of the “PALM” acronym may help with clinician recall of this new information, and it refers to the “PALM Scale” discussed in the literature. This PALM Scale is not really a classification of OSA but rather a method of characterizing the pathophysiological traits associated with airway narrowing and collapse (i.e., the reasons why the airway is closing).
Basically, individuals can present with different combinations of these traits that contribute to their OSA. It is rare for someone with OSA to be in one category only.
How is Obstructive Sleep Apnea Evaluated?
The gold standard for diagnosis of OSA is overnight polysomnography (PSG) that is reviewed by a sleep specialist (Becker et al., 2003). PSG includes multisystem assessment including electroencephalogram, electrooculogram, chin surface electromyography, single lead electrocardiogram, plethysmography using rib cage and abdominal bands, and nasal cannula or thermistor. The Apnea-Hypopnea Index (AHI) is a metric to quantify the severity of OSA (Berry et al., 2017). Apnea is classified as cessation of breathing for 10 seconds or greater along with respiratory effort, while hypopnea is a reduction of 30% or greater airflow (Berry et al., 2017). These events are tallied per hour of sleep, with more events related to greater OSA severity.
Click here for information on how swallowing is evaluated.
How is Obstructive Sleep Apnea Treated?
Continuous positive airway pressure (CPAP) is often employed as the first line of treatment. Other approaches include dental appliances (e.g., mandibular advancement), as well as surgical options for removal of extraneous tissues, including tissues of the uvula, palate and pharynx (i.e., uvulopalatopharyngoplasty). There has been an emerging interest in the use of hypoglossal nerve stimulation, which is a surgical implant that provides a constant electrical stimulus to the genioglossus muscle to maintain airway patency. Other adjuvant therapies include the use of sleep positioning (i.e., side-lying) and weight loss if obesity is considered a contributing factor.
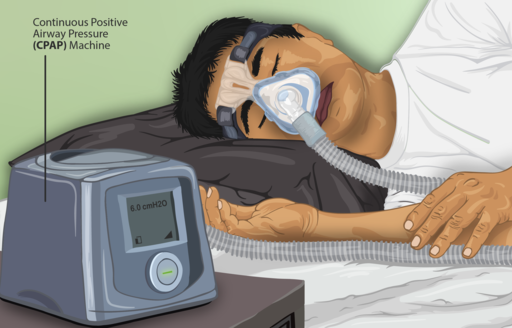
Continuous Positive Airway Pressure (CPAP) Machine. Creative Commons Attribution-Share Alike 4.0 International
In the last decade, especially in certain regions such as Brazil, Turkey, and portions of North America, oromotor exercises (aka, mouth and tongue exercises) and myofunctional therapies have been explored as a treatment option for OSA (Camacho et al., 2015; Carrasco-Llatas et al., 2021; da Silva et al., 2017; Guimarães et al., 2009). Specifically, clinical utility of lingual strengthening (e.g., Snoozeal®) (“New Clinically Proven Non-Invasive Treatment for Snoring,” 2020) has been investigated. Similarly, studies have also emerged regarding respiratory muscle strength training (Kuo et al., 2017; Vranish & Bailey, 2016).
People with Obstructive Sleep Apnea May Have Dysphagia
There have been reports of difficulty swallowing (dysphagia) in people with OSA, but the prevalence is wide, with a range from 16% to 78% (Bhutada et al., 2020). Common dysphagia findings were (Bhutada et al., 2020):
- delayed pharyngeal swallow response initiation (i.e., delayed swallow trigger),
- airway invasion (i.e., material penetrating into the top of the larynx or opening of the airway, which is called penetration; and dropping below the vocal cords, which is called aspiration),
- pharyngeal residue (i.e., food sticking in the throat), and
- impaired respiratory-swallow coordination (i.e., if you are breathing quickly, it may be difficult to squeeze in a time to stop breathing in order to complete a swallow).
Why are these swallowing difficulties occuring in people with OSA? The postulated risk factors for dysphagia in OSA relate to the sensorimotor alterations of the upper airway caused by the following (Friberg et al., 1998):
- low-frequency vibrations,
- intermittent hypoxia,
- frequent stretching, and
- inflammation.
Reduced upper airway sensations in OSA have been observed (Wallace et al., 2022). Individuals with OSA had impaired upper airway sensation to airflow, chemical, tactile and vibratory stimuli compared to controls. They also demonstrated reduced taste and smell.
Awareness & Education Needed Among Medical Speech Pathologists
Despite the high prevalence of OSA and risk of dysphagia, an international speech-language pathology (SLP) survey indicated limited knowledge about OSA and its pathophysiology (Wallace et al., 2021). Unfortunately, studies have not examined effects of behavioral intervention on swallowing-related metrics, although few demonstrate improvement in sleep quality-of-life measures and OSA severity.This begs for development of training and educational opportunities, as well as increased research efforts to further understand OSA impact on swallowing function and targeted efforts towards treatment. Until then, we encourage SLPs to collaborate with sleep physicians regarding our role in the interdisciplinary management of OSA.
Learn More: Obstructive Sleep Apnea & Dysphagia
- Webinar available through NortherSpeech.com for ASHA CEUs – Obstructive Sleep Apnea and Implications for the SLP
https://www.northernspeech.com/breathing-speech/dysphagia-in-obstructive-sleep-apnea-osa-an-under-recognized-impairment/
- SwallowYourPride Podcast 194 – Don’t Sleep on Sleep Apnea: The Link Between Swallowing & OSA by Kendrea L. (Focht) Garand PhD, CScD, CCC-SLP, BCS-S, CBIS, CCRE and Emma Wallace PhD
https://swallowyourpridepodcast.com/194-dont-sleep-on-sleep-apnea-the-link-between-swallowing-osa-kendrea-l-focht-garand-phd-cscd-ccc-slp-bcs-s-cbis-ccre-and-emma-wallace-phd/
Disclosure: SwallowStudy.com does not have anything to financially declare in relation to recommending this webinar and podcast.
How do I know I need a swallow study for dysphagia? How would a Speech Pathologist evaluate my swallowing?References for Obstructive Sleep Apnea:
Adler, D., & Janssens, J.-P. (2018). Estimating the probability of OSA in the spinal cord injury population: Specific tools are still needed. Thorax, 73(9), 803–805. https://doi.org/10.1136/thoraxjnl-2018-211954
Becker, H. F., Jerrentrup, A., Ploch, T., Grote, L., Penzel, T., Sullivan, C. E., & Peter, J. H. (2003). Effect of Nasal Continuous Positive Airway Pressure Treatment on Blood Pressure in Patients With Obstructive Sleep Apnea. Circulation, 107(1), 68–73. https://doi.org/10.1161/01.CIR.0000042706.47107.7A
Benjafield, A. V., Ayas, N. T., Eastwood, P. R., Heinzer, R., Ip, M. S. M., Morrell, M. J., Nunez, C. M., Patel, S. R., Penzel, T., Pépin, J.-L., Peppard, P. E., Sinha, S., Tufik, S., Valentine, K., & Malhotra, A. (2019). Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. The Lancet Respiratory Medicine, 7(8), 687–698. https://doi.org/10.1016/S2213-2600(19)30198-5
Berry, R. B., Brooks, R., Gamaldo, C., Harding, S. M., Lloyd, R. M., Quan, S. F., Troester, M. T., & Vaughn, B. V. (2017). AASM Scoring Manual Updates for 2017 (Version 2.4). Journal of Clinical Sleep Medicine: JCSM: Official Publication of the American Academy of Sleep Medicine, 13(5), 665–666. https://doi.org/10.5664/jcsm.6576 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5406946/pdf/jcsm.13.5.665.pdf
Bhutada, A. M., Broughton, W. A., & (Focht) Garand, K. L. (2020). Obstructive sleep apnea syndrome (OSAS) and swallowing function—A systematic review. Sleep and Breathing, 24(3), 791–799. https://doi.org/10.1007/s11325-020-02037-w
Camacho, M., Certal, V., Abdullatif, J., Zaghi, S., Ruoff, C. M., Capasso, R., & Kushida, C. A. (2015). Myofunctional Therapy to Treat Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. Sleep, 38(5), 669–675. https://doi.org/10.5665/sleep.4652
Carberry, J. C., Jordan, A. S., White, D. P., Wellman, A., & Eckert, D. J. (2016). Upper Airway Collapsibility (Pcrit) and Pharyngeal Dilator Muscle Activity are Sleep Stage Dependent. Sleep, 39(3), 511–521. https://doi.org/10.5665/sleep.5516
Carrasco-Llatas, M., O’Connor-Reina, C., & Calvo-Henríquez, C. (2021). The Role of Myofunctional Therapy in Treating Sleep-Disordered Breathing: A State-of-the-Art Review. International Journal of Environmental Research and Public Health, 18(14), 7291. https://doi.org/10.3390/ijerph18147291
da Silva, R. P., Martinez, D., Lopez, P., & Cadore, E. L. (2017). Effect of strength training on sleep apnea severity in the elderly: Study protocol for a randomized controlled trial. Trials, 18. https://doi.org/10.1186/s13063-017-2238-3
Eckert, D. J., & Malhotra, A. (2008). Pathophysiology of Adult Obstructive Sleep Apnea. Proceedings of the American Thoracic Society, 5(2), 144–153. https://doi.org/10.1513/pats.200707-114MG
Friberg, D., Gazelius, B., Lindblad, L. E., & Nordlander, B. (1998). Habitual Snorers and Sleep Apnoics Have Abnormal Vascular Reactions of the Soft Palatal Mucosa on Afferent Nerve Stimulation. The Laryngoscope, 108(3), 431–436. https://doi.org/10.1097/00005537-199803000-00022
Guimarães, K. C., Drager, L. F., Genta, P. R., Marcondes, B. F., & Lorenzi-Filho, G. (2009). Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. American Journal of Respiratory and Critical Care Medicine, 179(10), 962–966. https://doi.org/10.1164/rccm.200806-981OC
Jehan, S., Farag, M., Zizi, F., Pandi-Perumal, S. R., Chung, A., Truong, A., Jean-Louis, G.-, Tello, D., & McFarlane, S. I. (2019). Obstructive sleep apnea and stroke. 14.
Kuo, Y.-C., Song, T.-T., Bernard, J. R., & Liao, Y.-H. (2017). Short-term expiratory muscle strength training attenuates sleep apnea and improves sleep quality in patients with obstructive sleep apnea. Respiratory Physiology & Neurobiology, 243, 86–91. https://doi.org/10.1016/j.resp.2017.05.007
New clinically proven non-invasive treatment for snoring. (2020). British Dental Journal, 228(12), Article 12. https://doi.org/10.1038/s41415-020-1826-x
Tietjens, J. R., Claman, D., Kezirian, E. J., De Marco, T., Mirzayan, A., Sadroonri, B., Goldberg, A. N., Long, C., Gerstenfeld, E. P., & Yeghiazarians, Y. (2019). Obstructive Sleep Apnea in Cardiovascular Disease: A Review of the Literature and Proposed Multidisciplinary Clinical Management Strategy. Journal of the American Heart Association, 8(1), e010440. https://doi.org/10.1161/JAHA.118.010440
Vranish, J. R., & Bailey, E. F. (2016). Inspiratory Muscle Training Improves Sleep and Mitigates Cardiovascular Dysfunction in Obstructive Sleep Apnea. Sleep, 39(6), 1179–1185. https://doi.org/10.5665/sleep.5826
Wallace, E. S., Bhutada, M. A., Broughton, W. A., Eckert, D. J., & Garand, K. (2021). Knowledge, attitudes, and practice patterns of obstructive sleep apnea among speech-language pathologists. Sleep & Breathing = Schlaf & Atmung. https://doi.org/10.1007/s11325-021-02481-2
Wallace, E. S., Carberry, J. C., Toson, B., & Eckert, D. J. (2022). A Systematic Review and Meta-Analysis of Upper Airway Sensation in Obstructive Sleep Apnea – Implications for Pathogenesis, Treatment and Future Research Directions. Sleep Medicine Reviews, 101589. https://doi.org/10.1016/j.smrv.2022.101589
Zinchuk, A. V., Gentry, M. J., Concato, J., & Yaggi, H. K. (2017). Phenotypes in obstructive sleep apnea: A definition, examples and evolution of approaches. Sleep medicine reviews, 35, 113–123. https://doi.org/10.1016/j.smrv.2016.10.002
Thank You to the Guest Writers:

Dr. Ankita M. Bhutada is a speech-language pathologist and a clinician-scientist. She recently earned her Ph.D. from the University of South Alabama and was a part of the Swallowing Disorders Initiative Laboratory. Previously she worked as a senior speech-language pathologist in the Department of Physical Medicine & Rehabilitation and Kokilaben Dhirubhai Ambani Hospital, Mumbai, India. She is passionate about developing dysphagia-related clinical guidelines, assessment, and targeted interventions for medically complex conditions and underrecognized populations, including sleep-related breathing disorders. Her work has been funded by the Indian Federation of Neurorehabilitation and ASHFoundation. Contact Dr. Bhutada on Twitter: https://twitter.com/ankita_slp?lang=en
 Dr. Emma Wallace is a speech pathologist and Assistant Professor in the Discipline of Speech Pathology at the University of Sydney. She is passionate about clinical-research translation, evidence-based practice, and multi-disciplinary team collaboration. Her work has been funded by the Stroke Foundation and Sydney Health Partners. Emma has expertise in instrumental swallowing assessment and swallowing rehabilitation. She is the chair of the NSW branch at Speech Pathology Australia and a member of the Dysphagia Research Society. Contact Dr. Wallace:
Dr. Emma Wallace is a speech pathologist and Assistant Professor in the Discipline of Speech Pathology at the University of Sydney. She is passionate about clinical-research translation, evidence-based practice, and multi-disciplinary team collaboration. Her work has been funded by the Stroke Foundation and Sydney Health Partners. Emma has expertise in instrumental swallowing assessment and swallowing rehabilitation. She is the chair of the NSW branch at Speech Pathology Australia and a member of the Dysphagia Research Society. Contact Dr. Wallace:

Dr. Garand is an Associate Professor in the Department of Communication Science and Disorders at the University of Pittsburgh. She is the Principle Investigator and founder of the Swallowing Disorders Initiative Research Laboratory. She is currently the Vice Chairperson for the American Board of Swallowing and Swallowing Disorders. Her primary research interests include the impact of healthy aging and motor neuron disease on swallowing function. More recently, her work has expanded into investigating dysphagia in sleep-related disorders. Her work has been funded through the Veterans Affairs and ASHFoundation. You may find some of her scholarly publications in Dysphagia, Sleep and Breathing, Muscle and Nerve, Age and Ageing, and Journal of Speech, Language and Hearing Research.