
They Just Won’t Eat:
Instrumental Exams Allow for Person-Centered Evaluations,
Education & Counseling
By Katrina Woodward, MS, CCC-SLP, CDP, VP at SDX Dysphagia Experts
in collaboration with Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Looking back at my 20 years working as a speech-language pathologist (SLP) in skilled nursing facilities specializing in difficulty swallowing (dysphagia), I think about all the times I had to really dig deep to figure out a person’s underlying problems. Issues around aging and swallowing are so complex, and sometimes it was the people with dysphagia that I could not “fix” that were the ones I remember most fondly.
Why Did Ann Stop Swallowing?
Ann (name changed) was a lovely 80-something-year-old gal that loved to look at gossip magazines and boss around the nursing staff. She thought of us as her hired help. I was in my mid-20s back then and bonded with Ann over celebrity gossip and fashion faux pas. Her medical diagnoses that brought her to the subacute rehabilitation center only included: mild cognitive impairment (just a touch of memory loss), anxiety, and a TIA. Her older sister visited daily, but those visits seemed to only add to Ann’s “nerves.” I remember being in the room when Ann’s sister came calling, and it was like a switch flipped — like Ann wanted to be too sick to see her. Ann would start by ignoring her sister and then would literally panic, stop swallowing, and demand a Kleenex. This was NOT a one-time occurrence; this scenario repeated daily for a week straight. When Ann “forgot how to swallow,” she would go through a full box of Kleenex in an hour or two! She would repeatedly spit thin-clear secretions and wipe her tongue constantly, stating continuously that she could not swallow. I suspected it to be a psychogenic dysphagia, but she did not seem to show an actual fear of swallowing (i.e., phagophobia). I talked with Ann’s doctor and the nursing staff about her “spitting.” The behavior notably abated when Ann’s sister would leave. Ann could eat her meals but just not in the presence of her sister.
When she slept, she swallowed secretions. No coughing jags woke her in the middle of the night. Yet when her sister came to see her on her “sickbed,” Ann instantly transformed into a more anxious and tearful woman who could not swallow.
Of course, being a young dysphagia detective and curious as heck (about 3 years out of school then), I scoped Ann as soon as the doctor put in the order. Given her anxiety, I was initially on the fence with choosing FEES (Fiberoptic Endoscopic Evaluation of Swallowing) versus MBSS/VFSS (Modified Barium SwallowStudy.com/Videofluoroscopic SwallowStudy.com). However, Ann made the final decision, deciding she did not want to leave her room for love or money. So, I brought my FEES equipment into her room one day at breakfast, before her sister would arrive.
On her FEES exam, she swallowed fine. That is “within normal limits” fine! She could manage any food or liquid bolus with typical bolus control and containment and full bolus clearance. Nothing even came close to her airway, and she could cough and hold her breath like a champ. Even her secretion management was typical, and guess what? Saliva swallows at the onset of scoping occurred at the typical rate of approximately 2 per minute, and then at about 1 per minute.
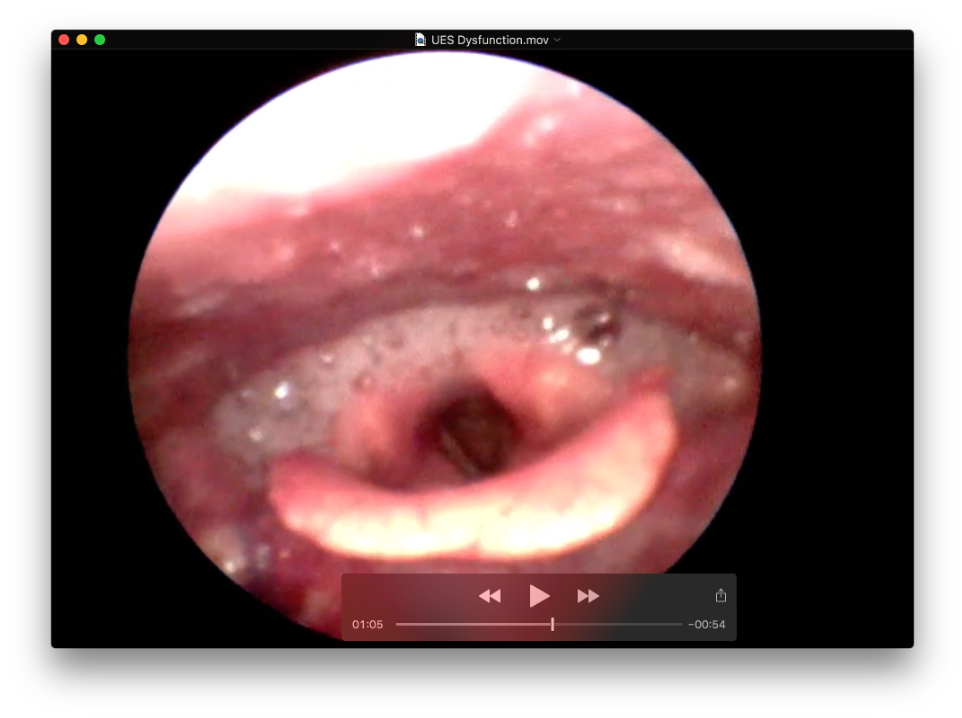
This is a FEES image that shows significant pooling of secretions in the pyriforms (aka, hypopharynx) and near the open laryngeal vestibule/airway. This was NOT Ann’s problem.
Even with a tube in her nose, her anxiety did not even kick in. She watched her actual swallows with curiosity. Additionally, with the biofeedback provided during the FEES, I proved to her that she could indeed handle her saliva, as well as food and liquid. The FEES provided her the necessary education and counseling in real-time.
She was referred back to her physician and psychiatry to manage this suspected psychogenic dysphagia. It clearly had a major trigger — Ann’s sister. Technically, Ann didn’t need me for dysphagia management. She did not have something I could treat with strengthening exercises, swallow strategies, or diet modifications. She needed her whole team to help her through the hardest part of each day without her sister’s visits pushing her over the edge and literally shutting her down. Family dynamics are a complicated piece of life, and although Ann never shared what was behind her need to be her sickest when her sister was present, her care team addressed the increased anxiety successfully. The psychiatrist saw her and began treatment for depression. Ativan was adjusted to a scheduled regimen, rather than being a PRN (as needed) medication. A couple of weeks later, Ann was more balanced, and she returned home with her sister. Her psychogenic dysphagia had disappeared at that time too. Significant weight loss was averted!
Now, I’m not advocating for magic little pills. I am stressing the need for speech-language pathologists (SLPs) and all staff to be invested in cases and people like Ann. Be an advocate. It was not one person who got to the bottom of the swallowing issues, it was the TEAM. And that team is made up of the person (as they are people first – not patients), family, nurses, certified nursing assistants, therapists (SLP/PT/OT), physicians, dietitians, the psychiatric service, and social workers. For other people with difficulty swallowing (dysphagia), the team may also include: otolaryngologists, gastroenterologists, neurologists, palliative care specialists, gerontologists, and more.
SLP as Detective
In retrospect, I did provide an integral piece of Ann’s care by giving the team the evidence to show that she had typical secretion management and a normal oropharyngeal swallow (oral and pharyngeal phases). That evidence from the instrumental examination was crucial before the team could take the next step in recognizing that there was a psychogenic dysphagia component to her problem swallowing. Because Ann was referred to me for swallowing difficulty, I became her “case manager” and her advocate. I was in the facility daily so I could track the situational problems (e.g., time of day and specific scenarios). Then I could relay my daily findings to the appropriate staff.

Sharing multiple accounts of her situational swallow dysfunction with the team contributed to the proper management and eventual resolution of her anxiety-driven psychogenic dysphagia.
In contrast to many cases I come across where a person won’t swallow or won’t eat, Ann’s case seemed very clear-cut. Now 15 years into my career as an SLP endoscopist (aka, an SLP who evaluates with endoscopy full-time), I’m often called in to perform a FEES to assess for a pharyngeal dysphagia component because a patient is complaining they can’t eat. Typically, weight loss is the main concern, and no overt signs or symptoms of aspiration are present at the bedside. In these cases where there isn’t a black & white solution to the suspected psychogenic dysphagia, using an instrumental exam is certainly appropriate to provide concrete evidence. Especially via FEES, you can assess for issues that often contribute to a person’s feelings of globus sensation (aka, lump in the throat) and the sensation that they cannot swallow. For example, you can assess for:
(1) suspected signs of gastroesophageal reflux and/or laryngopharyngeal reflux (LPR) by examining anatomical structures & viewing the laryngopharyngeal tissue;
(2) dry mouth (see tips # 7, 8 related to dry mouth in this blog), saliva quality, and secretion management. (Prior blogs linked in blue.)
I also ask:
- Why can’t they eat?
- Is “eat” a synonymous term for “taste?”
- Is “can’t” synonymous for “don’t want to?”
What may be behind the “They won’t eat” phenomenon?
Let’s brainstorm. Often, it’s not a singular cause but quite multifactorial. Investigation into potential psychogenic dysphagia requires a team approach, especially to rule-out all other causes. Did you know that iatrogenic causes are difficulties caused by the medical treatments themselves (e.g., side-effects of medications)?
1. APPETITE STIMULATION: APPEARANCE, TASTE & SMELL.
Yes, we eat with our eyes. Puree and baby food share a similar appearance and thus puree carries a negative connotation for many, often more for the family members than for the patient. But let’s focus on the patient without dysphagia and without an appetite…SMELL and appetite are interconnected. Did you know the following can impact your smell-ability: smoking, head and neck cancer with subsequent radiation treatment, nasal polyps, even a head injury? Collaborate with the kitchen and your registered (RDN) dietitian nutritionist in your facility to boost the sensory stimulation of the foods and drinks.
Talk with the nurses and medical team, as medications can impact taste too. For example, those that treat attention deficit hyperactivity disorder (ADHD): Adderall, Concerta, and Ritalin – give a bitter taste. Many common antibiotics (Penicillin, amoxicillin, Augmentin, Ancef, Keflex) affect zinc absorption and can leave a metallic taste if a zinc deficiency results. Lithium can also result in a metallic taste. See also this blog regarding medications and dysphagia.
2. BOWEL MOVEMENTS and appetite are also interconnected.
At our state ASHA conference in Connecticut in 2016, Dr. Paula Leslie, PhD, CCC-SLP, FRCSLT (from the University of Pittsburgh at that time & now from the University of Central Lancashire, UK) put it so politely in her British accent, calling bowel movements: “throughput.” If you have not heard that computer term, it refers to the amount of raw data that can pass through a system for processing. What it comes down to is if you are not pooping regularly, your system is not ready for a refill of raw material!
Think about all the things our patients are exposed to that impact their bowels: pain medications constipate, they are barely drinking enough fluids, they may have to use a bed pan, and they may not be moving around to get things going. That could certainly lead to a feeling of not being able to swallow (or psychogenic dysphagia). My advice: ASK your patient when they had their last bowel movement, or discuss this with the nurse and dietitian. If this one embarrasses you, don’t let it. I have learned that one thing most people who are older love to talk about is going to the bathroom. Ask, you’ll see!
3. ODYNOPHAGIA (aka, pain with swallowing) is an obvious one.
If there is complaint of pain with swallowing, then for sure that person will try to stop swallowing. The SLP will probably be pursuing an instrumental exam and/or follow up with ENT or GI depending on the locus of said pain. How do you capture pain? Wong-Baker my friends,
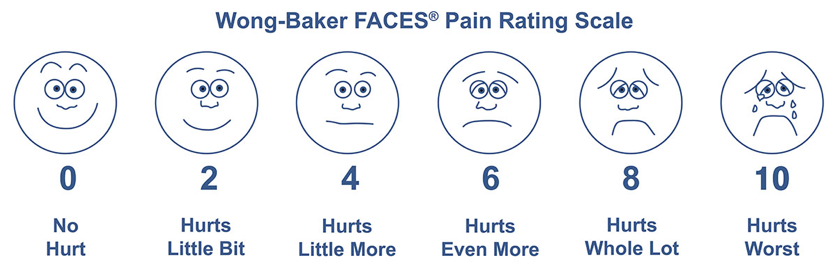
See https://WongBakerFaces.org
Wong-Baker Faces (i.e., the pain scale with emojis, before they were called emojis). Read more about pain scales. There is a tool for evaluating pain in people who are not able to express themselves and for people with dementia. It is called the PAINAD (click on it, print it, and use it). You want data? Rate the pain for solids, for purees, and for liquids. Now your bedside has data regarding the specific complaint to present to the physician and nursing staff.
Even if there are no signs or symptoms of aspiration, if someone tells me “A” is easier to swallow than “B,” then I document that and request the diet modification while the dysphagia workup continues. The important thing is to workup the pain with instrumental evaluation(s). Is it thrush, esophagitis, laryngopharyngeal reflux, GERD, a swallowed partial plate poking at their neck tissue (Karen had to add that one), or worse – a tumor/lesion?
People are not so accurate on localizing pain and food sticking. It is common for people to point to the neck area, when the issue is really in the esophagus (referred sensation). A VFSS with an esophageal sweep can identify where food is getting stuck, provide education/strategies (as these folks are often scared of choking), and make appropriate referrals. I find that about 50% of my FEES referrals for people with pain complaints and globus sensations actually have evidence of LPR. These people have a very high Reflux Finding Score and matching high Reflux Symptom Index (this second link reviews both scales).
Presenting those numbers along with the endoscopic images of the patient’s “angry throat” to the physician helps them take steps to treat the underlying cause of the odynophagia.
4. Do they have a DEPRESSION diagnosis? That is a big one.
Maybe the hardest hitter out of this list. There’s anxiety, major depressive disorder, adjustment disorder…all common terms heard in healthcare. In a skilled nursing facility, it is likely that half of the patients, whether living in a short- or long-term setting, have clinical depression (major depression), situational depression or significant depressive symptoms. A touching article by Dr Jules Rosen: A Doctor’s View: Depression in Long-Term Care Residents, discusses the importance of recognizing that medications do not solve all the problems. SOCIALIZATION during meals and activities combined with positive leadership helps buffer environmental changes. Socialization creates a reliable support network and gently facilitates this difficult transition. Imagine how hard it is going from being independent to being partially or fully dependent on others.
What is the appetite-depression connection? Well, we Americans are a stressed population! Long-term rises in cortisol & serotonin levels (both stimulate appetite) that accompany “low grade stress” will lead to weight gain. A short-term stress reaction (think acute illness) produces adrenaline which suppresses your appetite (think fight-or-flight survival mode). A change in weight means there is likely a change in appetite, and eating more or eating less can be an early sign of depression. In those with a previous depression diagnosis, a change in appetite can indicate a depression relapse. But why? Sometimes it is tied to a loss in energy or to a loss of interest for going out or for socializing. Transitioning to a skilled nursing setting, even when it’s a temporary situation, indicates that a person has lost control over some ability. Having to be dependent on others for tasks you were once self-sufficient at is frustrating, to say the least.
5. Other Related Diagnoses? ANOREXIA versus ARFID
Anorexia of Aging is an old term that I have heard through the years. It is not unusual in skilled nursing facilities to see an anorexia diagnosis before the Failure to Thrive diagnosis.
In many situations, a major-critical illness is often followed by reduced intake, protein energy malnutrition (PEM), and significant weight loss. All this can lead to sarcopenia (a loss of muscle mass and a decline in function with aging), which has been found to be associated with dysphagia (according to a meta-analysis by Zhao, et al. 2018). Sarcopenia was found to be an “independent risk factor” for dysphagia, per Maeda & Aka, 2016. (Fortunately, more researchers are looking at this connection; check out a PubMed search using “sarcopenia and dysphagia.”) So, the vicious downward spiral may begin. If an actual oral, pharyngeal and/or esophageal dysphagia did not start the issue of not eating, the person may develop dysphagia later due to the effects of sarcopenia and generalized weakness.
However, that older term of anorexia (or anorexia of aging) typically involves a body image disturbance (Zimmerman & Fisher, 2017), so we need to find a better term.
ARFID is a label that Karen Sheffler and I discussed as we were working on this blog. Avoidant/Restrictive Food Intake Disorder (F50.82) describes fears and avoidance issues, resulting in reduced intake even after a dysphagia has resolved or even when no dysphagia was noted. It is distinct from anorexia. It is a fairly new diagnosis, found in the DSM-5, and ARFID has no specific age limitations (Zimmerman & Fisher, 2017). It seems to better explain this pattern of poor oral intake in our older adults after hospitalization and institutionalization. I have yet to see it surface as a diagnosis in our skilled nursing facility patient population, but it certainly provides an improved specificity for post-illness onset of food-avoidance behaviors. Considering the trauma many elders go through during a critical illness, prolonged hospitalizations, intubations, adverse drug reactions, and other invasive procedures, it is a term that SLPs may become more and more familiar with as our geriatric population continues to grow.
To learn more on this ICD-10 diagnosis of ARFID, follow the links we provided above. However, please keep in mind, speech-language pathologists and all rehabilitation therapists do not diagnose these issues of psychogenic dysphagia, depression, anorexia, or ARFID, but we can be powerful advocates and make appropriate referrals to help solve our human puzzles. We are all beautifully complex puzzles.
Summary:
My grandfather, now 90 and still cognitively strong but bound to a wheelchair, once told me he was not afraid to have a stroke, he was afraid to survive it. I take this with me every time I meet a new patient. I’m there to give them support and answers and to share a smile. Don’t underestimate the power of positivity you can bring to a patient’s day with kind words and good listening. Be empathetic, but don’t be patronizing. Ask questions, listen, and wait for answers. Share a little bit of your life story and encourage your person you are evaluating/treating to do the same.
The takeaway from this article is three-fold:
1. Think OUTSIDE the BOX.
2. Use instrumentals FULLY, especially when a bedside / clinical evaluation does not paint the whole picture. And use instrumentals well. We can provide a lot of education and counseling with our powerful images. Don’t waste that opportunity to start the person’s journey to healing.
3. Think INTERDISCIPLINARY.
As an SLP, you are not just a therapist, you are a pathologist. You investigate, assess and make determinations. Your skill is not always to correct a problem. Sometimes it is to direct a situation down a different route. An SLP is an amazing person with critical thinking skills, patience, and a wide breadth of knowledge that (when not leaping buildings in a single bound) can create connections with other professionals to ensure that dysphagia complaints, whether related to the physical or the mental state, are addressed promptly & appropriately for patients across all levels of care.
THANK YOU TO MY GUEST BLOGGER:

Vice President of SDX Dysphagia Experts: Katrina Woodward, MS/CCC-SLP, Certifed Dementia Practitioner, is a FEES specialist who has worked in acute care, sub-acute, and long-term care facilities. Katrina is responsible for all aspects of SDX FEES and staffing business, including marketing/sales, special projects, customer service, educational networking events, and daily operations. Katrina was the 2016 recipient of the CSHA Distinguished Service Award. FOLLOW SDX on Instagram @SDXFEES.