
To Chin Tuck, or Not to Chin Tuck? That is the Question! Or is it?
By Karen Sheffler, MS, CCC-SLP, BCS-S of SwallowStudy.com
Introduction
In this article, I will attempt to address the many questions on this hot topic of: Is the chin tuck a universal safer swallowing strategy that can prevent aspiration?
First, we must ask:
- Are we advising patients to tuck, tilt, flex or look down?
- What do we call it?
- How do we teach it?
- What are the pros and cons of the chin tuck?
- Why are therapists prescribing it without an instrumental examination to prove that it works?
- Why has the chin tuck become so popular that many nurses and doctors are recommending it, sometimes without even referring the patient to a Speech-Language Pathologist?
No other safer-swallowing strategy or technique gets over-recommended as much as the chin tuck or chin down, or whatever you call it!
Every week on the job, I hear doctors and nurses instructing patients to use this very specific postural technique of tucking the chin when swallowing liquids. These professionals mean well and ultimately are trying to help prevent aspiration with liquids. (Aspiration is when material (like liquids) drop below the level of the vocal cords and into the airway or trachea that goes to the lungs.) However, making a recommendation without any evidence to support its efficacy is an unethical practice.
I will share evidence in this blog that the chin tuck/chin down posture may actually cause aspiration and worsen the swallow for some people with difficulty swallowing (dysphagia).
Yes, the chin tuck can make the swallow less safe!
The Modified Barium Swallow Study (MBSS, aka videofluoroscopic swallow study/VFSS) and the Fiberoptic/Flexible Endoscopic Evaluation of Swallowing (FEES) provide instrumental ways to evaluate the effectiveness of postural techniques. However, if a technique works once, the clinician should double check the effectiveness over at least 2-3 trials during that instrumental swallow study.
Clinicians better make sure that this safer-swallow technique works before we mandate someone look down all throughout a meal! Imagine being told to use a chin tuck every time you drink.
Here is a scenario to ponder to drive home this point: an 80 year-old ice hockey fan eats his dinner on a tray table in front of the TV. He takes a sip of his drink, tucks his chin down, hears “he shoots” coming from the TV, and while he swallows with a chin tuck, the TV shouts: “he scores!” Insert 4-letter word of choice. Good thing there is instant replay!
Why to use a Chin Tuck and/or Chin Down
(Per Welch et al., 1993 who used the term chin tuck; Logemann, 1993 who used the term chin down in her text; Shanahan et al., 1993 who used the term chin-down)
- Pushes the front (anterior) wall of the throat back to the back wall of the throat (pharynx)
- Pushes the tongue base and the epiglottis back
- May narrow the pharynx
- May help if tongue-base retraction is reduced, as the tongue base is closer to the back wall of the throat (posterior pharyngeal wall)
- Narrows the airway entrance (laryngeal vestibule entrance at the top of the airway or trachea)
- Widens the pocket that we naturally have behind our tongue (valleculae). Widening is in some people only.
- Increases probability material will sit in valleculae if the pharyngeal swallow is delayed. Shanahan et al., (1993) studied the chin-down posture in 30 patients with neurological impairment who had aspiration before the swallow. They noted that chin-down eliminated aspiration in only 50% of patients with a pharyngeal delay
- May reduce aspiration if the epiglottis is tilted backward and diverts material away from the top of the airway
More Research Cautiously Pro for Chin Tuck
- Bulow et al., (2001) tested patients with moderate to severe dysphagia. They found the chin tuck (“tuck the chin downward”) did not decrease the number of penetrations, but decreased the depth of penetration into the laryngeal vestibule/airway. But effortful swallow also decreased the depth of penetration. Chin tuck decreased the distance between the thyroid and the hyoid and between the mandible and the hyoid. However, no other videoradiographic or manometric measure was altered.
- Coyle (2014, April) noted that the chin tuck may work if the patient is having an oral containment problem with loss of the bolus to the pharynx in an unorganized way. Potentially, the chin tuck will contain the bolus anteriorly until the patient is ready to initiate the swallow. However, the patient better be able to eventually transport the bolus up and over the tongue; otherwise, the chin tuck would be detrimental.
- Macrae, Anderson & Humbert (2014) studied the duration of laryngeal vestibule closure (dLVC) with 16 healthy-young subjects, swallowing 5 times in a neutral position, 30 times in chin-down position, and 5 times again in a neutral position. Liquid was infused into the anterior oral cavity via a tube in 5ml amounts under videoflouroscopy. They used the term chin-down, but the instructions were: “tuck the chin to the chest.” However, they also used the word chin tuck in a chart on page 1253. (More on terminology differences in the last section of this blog). Significant findings:
- Chin-down swallows showed a longer duration of laryngeal vestibule closure by 94 ms. This is an increase by 20% compared with neutral swallows. This effect is likely due to the decreased distances as noted above by Bülow et al., (2001).
- Benefit was stable across 30 swallows, and this may be responsible for better airway protection in some people.
- Chin-down did not affect the pharyngeal swallow response, the speed of initiation of laryngeal vestibule closure, or the pharyngeal transit time while performing the posture.
- Chin-down had an after effect of increasing the pharyngeal transit time by 40ms on the final neutral swallows. This may make the chin-down potentially unsafe for some people, per the authors.
- Fraser & Steele (2012) studied two groups: 16 patients post-stroke and 26 heterogeneous patients from general medicine. Chin down was defined as a flexion of 76-77 degrees. Patients were instructed to “tuck their head downwards by looking down at their knees.” A positive effect was noted for cup drinking in both groups, eliminating penetration and aspiration in 11 patients. However, chin down worsened the patients’ swallowing safety when taking liquids by teaspoon, causing more deep penetration and aspiration than with the neutral swallow! Note: there were no cases of “normal” swallows without penetration when liquid administered by the clinician with a teaspoon, which may point to the importance of self-feeding small sips by cup.
“The fact that deterioration in swallowing safety was observed in this study to a substantial degree with teaspoon administration, and also in one case during cup drinking, provides evidence to support the current practice guidelines for S-LPs in Ontario, which state that postural modifications should not be prescribed without visual evidence of their benefit (College of Audiologists and Speech-Language Pathologists of Ontario, 2007).” (Fraser & Steele, 2012, page 147)
Why NOT to use the Chin Tuck/Chin Down
Logemann (1993, page 48) stated: “Some clinicians recommend this posture for all patients with dysphagia, but following this type of dictum can only lead some patients to increased difficulty in swallowing. The key to the successful use of posture to improve swallowing is to select the particular posture to match the individual patient’s physiology and anatomy.”
- Not appropriate for patients with decreased pharyngeal contraction (weak pharyngeal constrictors).
- Not for patients with reduced tongue control, per Logemann (1993).
- Not for patients with reduced anterior to posterior oral transit.
- Not for patients with poor lip closure.
- Chin tuck does not change the dimensions of the pyriform sinuses.
- Will not eliminate aspiration if the pharyngeal delay is significant enough and the bolus volume is large enough to spillover out of the valleculae and into the pyriforms (Shanahan et al., 1993). The chin tuck cannot prevent aspiration of the food/liquid dumping out of the pyriforms and into the airway. Coyle (2014) advised against blindly using the chin tuck/chin-down by referring to Shanahan’s 1993 research. Here we are 22 years later, still reminding everyone that the chin tuck is NOT for all patients.
- Coyle (2014) stated the chin tuck is also detrimental if the patient aspirates due to residue in the pyriforms, as the chin tuck may dump residue into the airway
More Research Con for the Chin Tuck
- Bülow et al. (1999) found negative effects on pharyngeal peak pressures and contraction durations during chin tuck.
- Bülow et al. (2001) noted the chin tuck did not improve weak pharyngeal constrictor muscles and did not change the amount of residue in the pharynx.
- Bülow et al. (2002) found there was no improvement in intrabolus pressure when a patient performs a chin tuck. These 8 patients (6 CVA and 2 head and neck cancer) already had significantly reduced pharyngeal constrictor activity. “Intrabolus pressure at the level of the inferior pharyngeal constrictor is highly dependent on an effective peristaltic contraction wave (page 199 ).” The chin tuck does not facilitate pharyngeal contraction.
- Hori et al. (2011) found that the chin tuck requires more lingual effort to apply tongue pressure to drive small boluses (5ml) posteriorly in young healthy subjects. No influence was found on 15ml swallows.
- Balou et al. (2014) found the chin tuck has minimal effect on pharyngeal pressures or UES relaxation. Peak pressures increased slightly with a chin tuck in the valleculae and decreased slightly in the pyriforms. Overall duration of contractions increased, but the onset of contraction was slower with the chin tuck. The chin tuck caused the pharyngeal muscles to take longer to contract. This supports Bulow’s findings that if the patients pharyngeal constrictors are already weak, the chin tuck is worse. Furthermore, chin tuck and chin down reduced the duration of UES relaxation. One positive function of the chin down and chin tuck was to reduce UES residual pressure (with chin down being better than chin tuck). However, the head rotation was much better at decreasing UES residual pressure, with even a partial head rotation better than nothing. Unfortunately, though, this research was with conventional manometry and with only a 3ml bolus size in 10 healthy adults.
- Terre & Mearin (2012) found that the chin down maneuver only prevented aspiration in 55% of the patients with TBI and CVA. Specifically, the following dysphagia characteristics caused the patients to not benefit from chin down:
- more severe dysphagia,
- aspirating even with small bolus volumes,
- significant pharyngeal delay,
- pharyngeal residue, and
- cricopharyngeal dysfunction.
- McCulloch et al. (2010) studied 7 young healthy subjects with High-Resolution Manometry (HRM). They analyzed: neutral swallow, head turn to the same side as catheter placement, and chin tuck with 5ml boluses, 5 times per head position. Note: HRM provides much better data to evaluate pressures along the pharynx and across the pharyngoesophageal segment (PES). It has more sensors tightly spaced across the PES than traditional manometry, and this is crucial as the area moves superiorly as much as 4 cm, per McCulloch et al., (2010).
Summary of results for chin tuck (*caution with interpretation, as this was a very small sample):
-
- No effect on maximum velopharyngeal pressures.
- No effect on tongue base maximum pressure. Maximal tongue base pressures were the highest with neutral position swallows.
- No change in rate of pressure rise and no change in pressure gradients (Pressure gradient: takes data on the sensor that shows the maximum pressure and then compares that with the pressure at 1-2 cm distally at the same point in time).
- Duration of tongue base pressure to the pharyngeal wall was shorter for the chin tuck, but longer for the head turn.
- Pre-swallow peak UES pressure was greater for neutral swallows versus head turn. Chin tuck did not reach significance.
- Chin tuck caused lower post-swallow peak UES pressures
- Minimum pressure during upper esophageal sphincter (UES) opening was higher for chin tuck and lower for head turn, but these did not reach significance.
- Chin tuck appeared to increase UES opening time, but it did not reach significance.
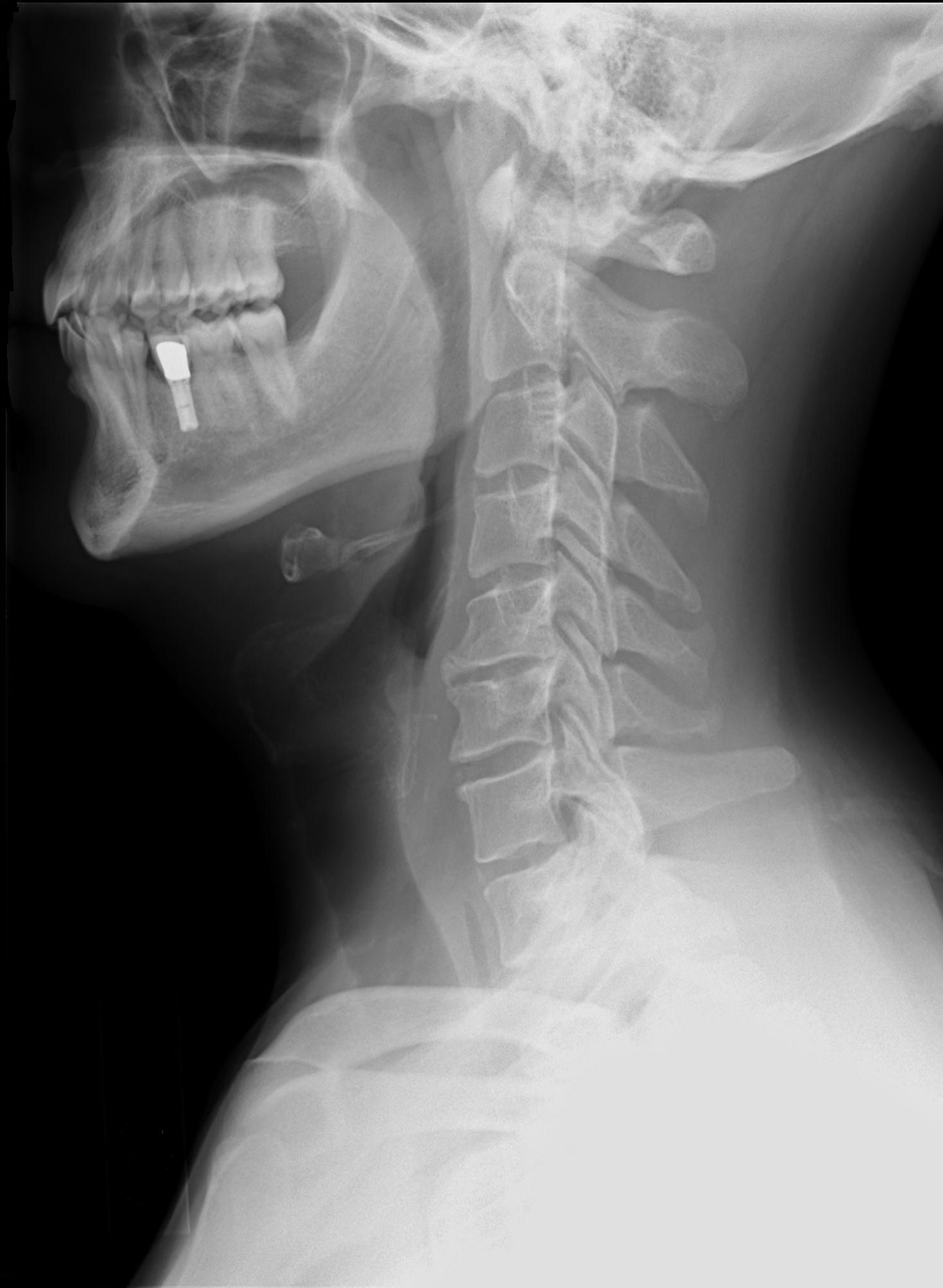
This is a neutral position. Not a chin tuck or chin down posture.
Chin Tuck versus Chin Down — “What’s in a name?”
Look at the array of descriptions for this postural technique:
- Chin tuck
- Chin-down
- “Tilting the head forward, chin down,” as written by Logemann (1993).
- Head Flexion
- Head Down
- Chin downward looking at knees
- Chin to neck
- Chin to chest
- Chin lowered maximally
- Tuck you chin as close to your sternum as possible.
Many people have used the terms chin tuck and chin down interchangeably. Per Okada, et al., (2007) there is poor agreement among Speech-Language Pathologists (SLPs) about how to teach this maneuver and how to define differences between chin tuck and chin down. Okada’s team noted only 58% of SLPs from the US and 23% of SLPs from Japan even make a distinction between chin tuck and chin down.
The following new research suggests we should be paying attention to the distinctions.
Hot of the presses: Leigh et al., (2015) studied the difference between Neutral posture, Chin-Down and Chin-Tuck in 40 healthy adults from 26-79 years of age. Unfortunately, this study analyzed only one swallow per posture to limit flouroscopy/radiation time, and the 10ml boluses were given by spoon. Subjects were provided pictures along with these descriptions:
Chin-down (DOWN): “move your chin down;” “comfortable chin-down.”
Chin-tuck (TUCK): “tuck you chin as close to your sternum as possible;” “intentionally bring or touch your chin to your chest.”
TUCK was more effective than DOWN in the following aspects:
- Shorter distance between epiglottic base and the arytenoids
- Narrower anteroposterior diameter of the laryngeal entrance
- Shorter distance from the epiglottic base to the posterior pharyngeal wall
- Greater backward retraction and elevation of the epiglottic base, which is a marker for the tongue base (2D displacements/excursions).
- TUCK may enhance tongue base retraction, but the DOWN posture does not (per the authors’ conclusions).
Unfortunately, with the swallow in motion, some negative impacts of the TUCK were:
- Restricted maximal horizontal excursion for the hyoid bone, epiglottic base, and larynx. This may be due to compression of the submental muscles or due to a decreased resting muscle length, per the authors. Would this decrease UES opening in some patients?
- Peak velocity of horizontal movement of the hyoid bone was reduced.
- Both TUCK and DOWN reduced vocal cord motion during swallowing when compared to the neutral posture. DOWN reduced the vertical and horizontal displacements of the vocal cords. TUCK limited the horizontal movement of the vocal cords. However, distances are shortened in the TUCK posture, so the posture may still offer some airway protection despite reduced hyolaryngeal excursion.
The DOWN posture had no effect on the anteroposterior pharyngeal or laryngeal inlet distances. DOWN restricted the vertical and horizontal laryngeal excursion, but had no effect on hyoid bone movement.
A positive effect of the DOWN posture was that the horizontal excursion of the epiglottic base was increased, which this may be consistent with opening the valleculae space as noted above.
Summary on Chin Tuck and Chin Down: Do they make the swallow safer?
I’m very concerned about this recent trend I have seen in healthcare where well-meaning professionals are telling patients to use a chin-down or chin-tuck without knowing the evidence and without seeing if the strategy works based on instrumental assessments. It is only one technique or strategy out of many that the SLP evaluates during an instrumental exam.
Is it ethical for a surgeon to tell a person who just had thyroid surgery: “just tuck your chin, especially with liquid,” rather than consulting an SLP who specializes in swallowing? A real person was told this by a surgeon during her post-operative follow-up after she complained of difficulty swallowing liquids safely. Her surgery was a challenging removal of a large thyroid tumor that sacrificed the recurrent laryngeal nerve on one side (nerve that closes up the vocal cords for voicing and swallowing). Clearly people need to advocate for themselves and ask to be seen by a specialist in swallowing.
Given the information above, the chin tuck and chin down can reduce vocal cord movement, will have no impact on the weakness in the hypopharynx at the level of the pyriforms, and a person may have increased aspiration out of the pyriforms. A chin tuck would likely do her more harm than good.
Terre and Mearin (2012, page 419) cautioned: the chin tuck/chin down is “not universally applicable to all dysphagic patients.” Additionally, if the actual chin tuck posture is better than the chin-down posture “swallowing in (that degree of) cervical flexion can be uncomfortable.”
The chin tuck and chin down posture are not magic bullets defeating aspiration. At least 50% of the time the strategy will not work. This cannot be confirmed at the bedside without an instrumental exam. We might as well flip a coin for “Heads = Chin tuck, Tails = no chin tuck.”
All joking aside, the scary aspect is that the chin tuck may cause much more aspiration than swallowing in a neutral position for some people. If the person has moderate to severe dysphagia, they will also likely be silently aspirating. Therefore, the nurse may think the chin tuck is working, while the patient ends up silently aspirating even more.
Bottom line:
Consult an SLP to
View it before you use it!
References
Balou, M, McCullough, GH, Aduli, F., Brown, D, Stack Jr, BC, Snoddy, P & Guidry, T. (2014). Manometric measures of head rotation and chin tuck in healthy participants. Dysphagia, 29, 25-32.
Bülow, M, Olsson, R, & Ekberg, O (2001). Videomanometric analysis of supraglottic swallow, effortful swallow, and chin tuck in patients with pharyngeal dysfunction. Dysphagia, 16 (3), 190-195.
Bülow, M, Olsson, R, Ekberg, O (2002) Supraglottic swallow, effortful swallow, and chin tuck did not alter hypopharyngeal intrabolus pressure in patients with pharyngeal dysfunction. Dysphagia, 17, 197-201.
Coyle, J.L. (2014, April). IIS5: Dysphagia Interventions: Are We Treating the Bolus, the Patient, or Something Else? Seminar presented at the Healthcare & Business Institute of the American Speech-Language-Hearing Association, Las Vegas, NV.
Ekberg, O (1986) Posture of the head and pharyngeal swallowing. Acta Radiol Diagn (Stockh) 27, 691-696.
Fraser, S & Steele, CM (2012). The effect of chin down position on penetration-aspiration in adults with dysphagia. Canadian Journal of Speech-Language Pathology and Audiology, 36 (2), 142-148.
Hori, K., Tamine, K., Barbezat, C., Maeda, Y., Yamori, M., Muller, F. & Ono, T. (2011). Influence of chin-down posture on tongue pressure during dry swallow and bolus swallows in healthy subjects. Dysphagia, 26 (3), 238-245. doi: 10.1007/s00455-010-9292-2
Leigh, JH, Oh, B, Seo, HG, Lee, GJ, Min, Y, Kim, K, Lee, JC & Han, TR. (2015). Influence of the chin-down and chin-tuck maneuver on the swallowing kinematics of healthy adults. Dysphagia, 30, 89-98.
Logemann, JA (1993). Manual for the Videoflourographic Study of Swallowing: Second Edition. Austin, TX: Pro-Ed.
Logemann, JA (1998). Evaluation and treatment of swallowing disorders. Austin, TX: Pro-Ed.
Macrae, P, Anderson, C & Humbert, I. (2014). Mechanisms of airway protection during chin-down swallowing. Journal of Speech, Language, and Hearing Research, 57, 1251-1258. doi: 10.1044/2014_JSLHR-S-13-0188
Okada, S., Saitoh, E., Palmer, JB, Matsuo, K., Yokoyama, M. Shigeta, R. & Baba, M. (2007). What is the chin-down posture? A Questionnaire survey of Speech-Language Pathologists in Japan and the United States. Dysphagia, 22 (3), 204-209. doi: 10.1007/s00455-006-9073-0
Shanahan, TK, Logemann, JA, Rademaker, AW, Pauloski, BR, Kahrilas, PJ (1993) Chin-down posture effect on aspiration in dysphagic patients. Arch Phys Med Rehabil 74, 736-739.
Updated Reference:
I love this article! I am an SLP in acute inpatient rehab. I am creating a in-service for nursing. One of the topics I would like to discuss is why chin tucks are NOT always appropriate for the patient. Do you have any visuals such an VFSS that shows a person who is NOT appropriate for a chin tuck? Visuals are always helpful in teaching others – especially nursing who doesn’t see VFSS regularly. I am showing a variety of VFSS demonstrating a range of deficits, but I can’t recall a particular recent VFSS where I trialed a chin tuck and it was deemed to be inappropriate. I tried going through all of the VFSS files but there are so many and it is hard to recall which one I trialed a chin tuck with and which I didn’t. Thanks in advance!
Thanks!
Yes visuals speak a thousand words. It would be great to have a video clip of the chin tuck causing aspiration. I have seen that in action, but don’t have a video clip immediately available to send to you.
You could show images of when someone has a lot of pharyngeal residue, especially pyriform residue. The audience can see then how a chin tuck would be detrimental if residue flows out of pyriforms and into airway.
See also the bullet points in the blog above for when the chin tuck may NOT work.
You could also demonstrate how a person with weak tongue and lip control would have the bolus fall out of the mouth if the chin was down. That would be a funny demo of you with a cup to catch your anterior spillage!
I have a talk coming up on SpeechPathology.com – June 8th 12-2pm EST on videofluoroscopic swallow studies. In that I will be talking about timing abnormalities associated with aspiration. One of these is “Prolonged Pharyngeal Bolus Dwell Time” – or how long does the bolus hang out in the pharynx with the laryngeal vestibule wide open. You can imagine if this material is hanging out in the hypopharynx and the person tucks their chin, that material could fall forward to the airway.
(Morton, et al., 2002). Morton et al found that aspiration especially occurs when paired w/ inspiration after the swallow and/or irregular breathing.
Is chin tucking appropriate for treating forward head posture?
Can you please explain “forward head posture,” and how and why are you treating that head posture? Do you mean that the person is unable to hold his/her head up?
In general the use of a chin tuck as a means to prevent airway penetration and aspiration needs to be tested with an instrumental evaluation, such as a videofluoroscopic swallow study or a FEES. You have to make sure that the chin tuck posture itself does not make the swallow worse (less safe) and cause more aspiration.
I have colleagues who would recommend chin tuck at bedside and evaluate its effectiveness by lack of overt signs of aspiration (coughing/choking/wet voice). Personally I may trial it at bedside but would not use it as a recommendation unless I had an instrumental assessment with chin tuck. However, I can see their rationale as well. If it is not the best practice, I’m just a bit concerned as newly qualified SLPs may be learning from such practice.
It is tough as a new clinician seeing older clinicians who may be very set in their ways do things that are not fully supported in our evidence/literature. You are accurate that we only know that a strategy is for sure safe and effective by doing an instrumental evaluation. That being said, in these days of COVID-19 and lack of safe access to instrumentals, we do have to use our best clinical judgement and look at the big picture too. Talk with the person’s medical team. Is taking a risk with someone right now prudent, especially if there is a high risk for silent aspiration (i.e., elder, dementia, prior dysphagia, prior Neuro issues, and/or prior head/neck CA issues, hx of COPD, etc) and if there is a high risk for reintubation and other negative sequela. I always keep in mind this Miles, Anna research (from New Zealand) (2018) https://www.ncbi.nlm.nih.gov/pubmed/29845700 — where she found that often people cough with thin liquid presentation and go on to silently aspirate the next nectar thick/mildly thick liquid presentation. What if that person you are talking about overtly aspirates the big sip of thin liquid, but then goes on to aspirate the next sip with the chin tuck — and we perceive that lack of cough as “tolerating.” Miles found: “Cough response to aspiration differs across bolus volumes and viscosities,” therefore, a person is not simply an overt aspirator or a silent aspirator. Their cough response to two different aspiration episodes can be vastly different. This is why now with COVID19 and the lack of instrumentals — we really have to try our best, knowing that this is not a perfect situation. Please also see my new blog on post-extubation dysphagia and all the resources there. Thanks for your comments! Keep questioning!
Although the CTM is widely used to prevent aspiration in patients with dysphagia, some studies question its effectiveness. An evidence-based systematic literature review on the impact of dysphagia treatment on populations with neurological disorders found that CTM was effective in 8 to 50% of cases. In a study involving patients with Parkinson’s disease and dementia, CTM was less effective when compared with the intake of thickened liquids.
I agree that the chin tuck is less than 50% effective and needs to be individually tested with instrumental exams to prove that it works to reduce or prevent aspiration. Could you please provide citations for your specific points mentioned above? Thanks