
This oral hygiene blog was inspired by the presentation:
“Dental Perspectives on Aspiration Pneumonia Causes and Management”
by Kennneth Shay, DDS, MS
Dentist and Gerontologist
Department of Veterans Affairs: Office of Geriatrics and Extended Care
ASHA Healthcare & Business Institute
April 12, 2014

The biggest hole in the body can harbor many bacteria.
“The mouth is dirty,” Dr Kenneth Shay stated frankly at the ASHA Institute, and it’s “the biggest hole in your body!”
Warning: You may want to finish eating, brush your teeth, floss, use mouthwash, and then come back…
If it is early morning and you haven’t brushed your teeth yet, then scrape the gunk off your teeth with your fingernail. You may have found 10 billion microorganisms in that one cubic millimeter.
There are 1 trillion to 10 trillion microorganisms in your mouth.
Simply brushing your teeth can get rid of that nasty bacteria film in your mouth. It can also prevent “some of that schmutz” from getting into your lungs, reminds Shay. If you are having trace aspiration (saliva, food, and/or liquids getting into your lungs), try to make what gets into your lungs less nasty. You can prevent pneumonia.
Pneumonia that is due to poor oral hygiene and poor oral care is a major avoidable infection, per Shay.
Ross & Crumpler (2007) noted:
“despite strong evidence in the literature on the role of oral care …, nurses continue to view oral care as a comfort measure with low priority and utilise foam swabs rather than toothbrushes.”
“Toothette sponges are wimpy,” stressed Shay. They don’t get the gunk (plaque) off the teeth. Plaque is sticky. The best mouthwash alone does not cut it. Brushing the teeth is necessary. This scrubbing action provides 90% of the necessary cleaning, per Shay.
Why is oral hygiene & the mouth forgotten in healthcare?
We wash our hands and wear gloves before serving food to prevent spreading harmful bacterial infections. So why not brush the teeth of a dependent elder in order to prevent a bacterial pneumonia?

We help dependent elders with many activities of daily living. Brushing the teeth is just as important as bathing and dressing.
We help him go to the bathroom many times a day. So why don’t we help brush his teeth?
I’ve heard some medical personnel say they are squeamish about the mouth. It makes them gag!
Well, we should be gagging over the medical costs of neglecting the mouth.
This simple prevention technique of brushing the teeth costs pennies a day against the cost of a pneumonia. Based on CDC numbers from 2011, there were 157,500 Health Care Associated Pneumonia (HCAP) infections that year. CDC states the average added cost of one HCAP is $22,875. This equals over 3 billion dollars annually on preventable infections!
See: https://www.cdc.gov/hai/surveillance/
Shay also speculated that one reason why the mouth is the forgotten part of medicine is that the medical profession began to ignore it about 150 years ago. This was when the dental profession split from the medical profession. Then to make matters worse, in 1965, dentistry said “no thank you” to Medicare.
How does the bacteria grow in there in the first place?
Imagine your mouth as a parking lot with the parking spaces being between the tooth and gum (called gingival spaces). There are a lot of parking spaces for the germs in these 1-3 millimeter deep crevices. If germs park in the gingival space for more than 24 hours, they become calcified into plaques. Bacterial loves to stick to it. Brushing removes plaque. No brushing leads to a build-up of plaque in the gingival space and inflammation (gingivitis).

Gingivitis – red, inflamed gums. Clears up with good brushing, improved oral hygiene and oral infection control. Brush off the plaque before it becomes calculus.
It only takes 48 hours of hospitalization in a critically ill patient to change the bacteria from the usual gram-positive streptococci to gram-negative microorganisms (nasty pathogenic bacteria that cause pneumonia).
Maybe our patients’ teeth are not brushed because the gums bleed? Blood is okay, per Shay, even if you are on a blood thinner. Shay stated that bleeding is a sign that you need to brush more. It is due to the inflammation from gingivitis, but regular brushing will eliminate the bleeding. Shay warned that bleeding is only risky if the patient has a blood disorder or disease that causes excessive bleeding.
Most cases of gingivitis do not progress to the more serious periodontitis or to pneumonia.
Immune compromising events can cause an autoimmune response. This may cause gingivitis to progress to periodontitis. Immunocompromising events are not only hospitalizations and critical illnesses, but also the following examples:
- life stressors,
- flu,
- depression, and
- pregnancy.
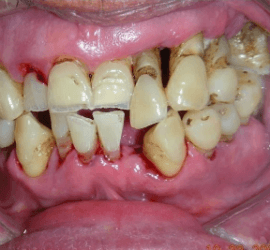
Periodontitis with gums receded and more space for the gram-negative bacteria to colonize surfaces.
Periodontitis is inflammation caused by bacteria that affect the attachment between the tooth and the bone. It is an irreversible destruction of the supporting tissues (periodontal ligament to alveolar bone). Shay explained how bone-absorbing cells can then eat away at the bone. The bone will not be regenerated. Additionally, as the gums recede and the bone wears away, the cementum is exposed. Cementum is not hard and smooth like enamel. It is rough, and bacteria can stick to it easier than enamel. Cementum has a higher organic content, and is more susceptible to decay when there are changes in salivary pH.
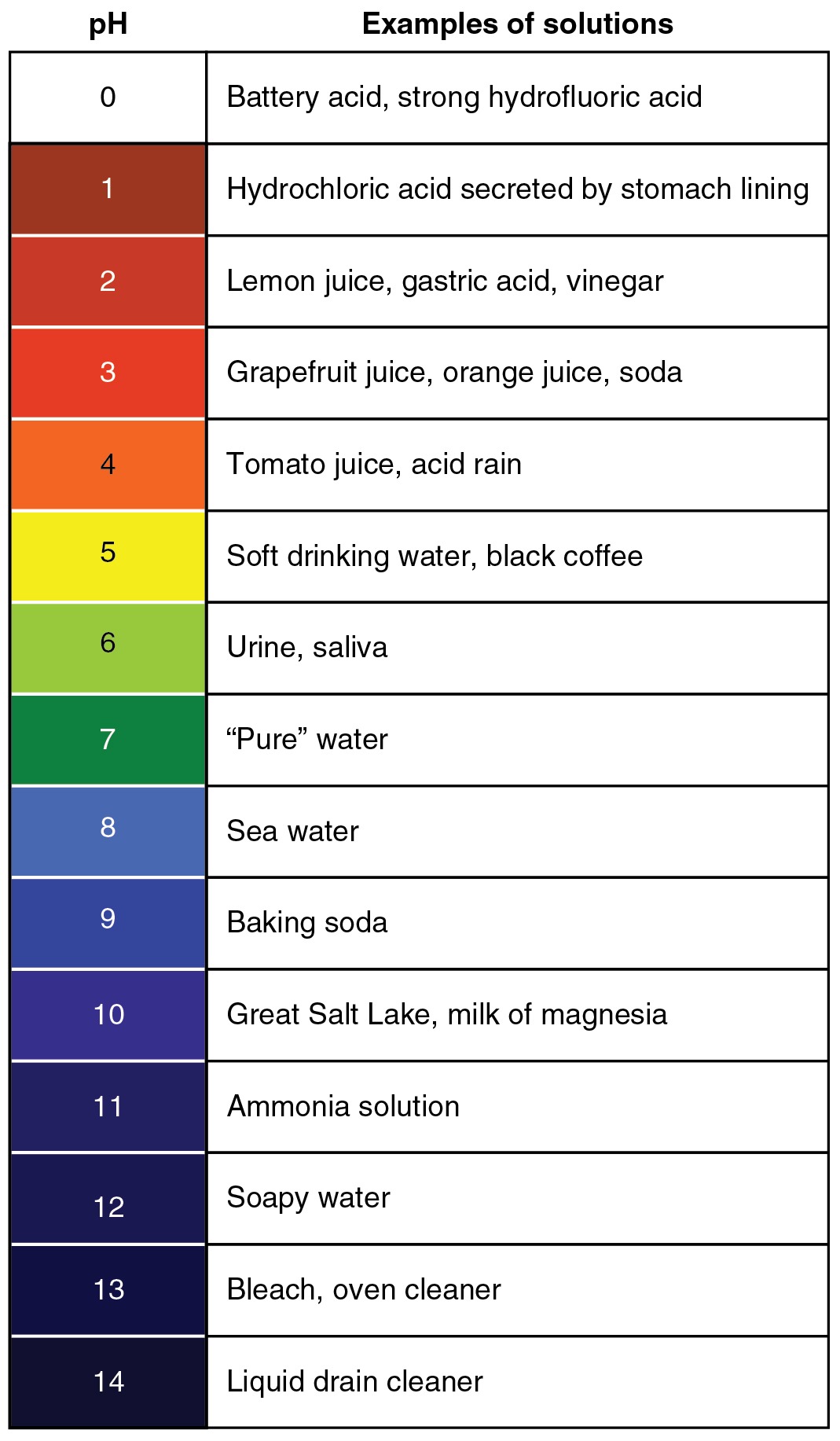
pH Scale. Note how pH of saliva should be a fairly neutral 6. Read more about saliva here.
The periodontal pocket creates a larger parking garage that can be up to 6-8 millimeters deep.
Now “there is more surface area to collect gunk,” per Shay. Even more gram-negative anaerobes can park there!
“These are the same things that cause aspiration pneumonia,” stated Shay.
********
Thank you for reading and sharing. This was Part 1 of my series on
Oral Hygiene & Aspiration Pneumonia Prevention.
My blog series will provide more information on salivary changes that happen in critically ill individuals, dry mouth, the complexity of saliva, the transport of colonized bacteria/pathogenic organisms from mouth to the lungs and through bloodstream, and oral infection control/oral hygiene protocols.
Jump forward to Part II, Part III, Part IV, “It’s Alive: Oral Microbiome”, & Saliva Puzzle.
See my FREE webinar on Oral Infection Control the National Foundation of Swallowing Disorders (NFOSD) website: https://swallowingdisorderfoundation.com/webinar-oral-care/
See also Oral Infection Control / Oral Care Procedures (PDF included), which should be documented as “oral infection control” or “oral decontamination for aspiration pneumonia prevention.”
Thank you for reading and sharing. Hope this helps your facility create evidence-based policies.
thanks, let me know if you have questions